Penetrating injury
Contrast extravasation or false aneurysm formation
Adventitial or medial tear without an intimal injury
Blood flow deviation due to large hematoma, or vascular spasm
Blunt injury
Caused by vascular compression and stretching
All vascular layers tear can occur, as well as an intramural hematoma
Dissection, occlusions or vessel rupture in severe injuries
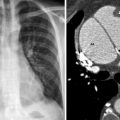
Blunt aorta injury
Blunt aortic trauma is fatal in ascending aorta (die at scene of accident)
Signs of mediastinal hematoma on chest radiograph or scout CT view
Hepatic and splenic injury
(CT diagnosed) Extravasation point or blush of contrast overlying/surrounding the organ
Renal injury
(CT diagnosed) Angiography not always indicated unless persistent hematuria, or contrast extravasation on delayed imaging (e.g. plain KUB)
Pelvic injury
Pelvic fractures associated with massive blood loss (venous injury).
Arterial injury can also occur with extravasation, pseudoaneurysm and AV fistula formation
Angiography can show persistent bleeding following pelvic fracture stabilization/fixation
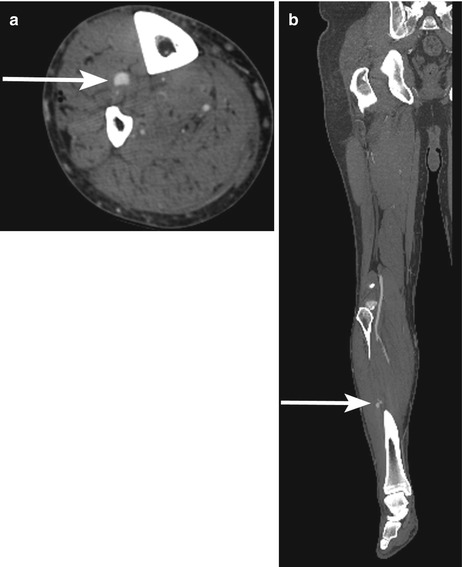
Extremity injury
Direct limb trauma or dislocation (e.g. the popliteal artery)
Angiography can show dissection, occlusion or disruption in blunt injury
Extravasation, pseudoaneurysm or AV fistula formation in penetrating
Computed Tomographic Angiography
The availability of CTA has increased and it has become standard in most tertiary trauma centers (Fig. 39.1a, b). CT consoles and picture archiving and communication systems (PACS) can complement CTA images of a trauma patient with automatic generation of a series of multi-planar reconstructions (MPR) for bony, visceral or vascular injuries in 3 dimensional planes.