Vasculitis and Vasculitides
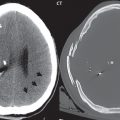
Sickle Cell Disease
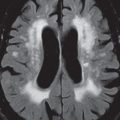
There is a high incidence of infarcts in patients with sickle cell disease, with these commonly watershed in distribution. Clinically silent lesions, ischemic in etiology, are noted in deep white matter, with the MR appearance consistent with gliosis ( Fig. 1.75 ).

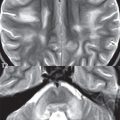
Moyamoya Disease
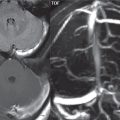
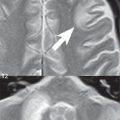
In Moyamoya disease there is marked stenosis and/or occlusion of the terminal internal carotid arteries, together with the proximal anterior and middle cerebral artery branches. An extensive network of small collateral arterial vessels develops at the base of the brain, involving the lenticulostriate and thalamoperforating arteries (the “cloud of smoke” on angiography). Moyamoya is predominantly a disease of children, with an increased incidence in the Japanese and Korean populations, and relentless progression. MR reveals the multiple tiny collaterals, as flow voids, both in the basal ganglia and within enlarged CSF spaces ( Fig. 1.76 ). MRA and CT angiography (CTA) reveal the narrowing of the supraclinoid internal carotid arteries, and preferential vascular disease involving the anterior circulation. Collateral vessels from the extracranial circulation (external carotid artery) may also be visualized. Multiple, bilateral hemispheric and deep white matter infarcts may be present, predominantly in the carotid distribution and in watershed regions. Surgical treatment of moyamoya includes both direct and indirect revascularization.

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


