Wilms Tumor
 BACKGROUND
BACKGROUND
What is the estimated annual incidence of Wilms tumor (WT) in the U.S.?
∼500 cases/yr of WT are diagnosed in the U.S.
What is the median age at Dx?
Median age at Dx is 3–4 yrs (95% <10 yrs) for WT.
Is there a sex predilection?
Yes. Females are more commonly affected than males.
How does the age of presentation differ with Wilms when compared to neuroblastoma (NB)?
NB often presents at <2 yrs. Unilateral WT presents at 3.5–4 yrs.
What is the age of presentation for hereditary/bilat tumors?
Hereditary/bilat tumors often present at 2.5 yrs (younger than sporadic cases).
Name 3 genetic syndromes associated with Wilms.
1. WAGR
2. Denys-Drash
3. Beckwith-Wiedemann
What is WAGR syndrome, and what is the associated genetic change?
Mnemonic: WAGR:
Wilms
Aniridia
GU anomalies
Mental Retardation
Associated genetic change: del 11q13 (WT1 deletion)
What is Denys-Drash syndrome, and what is the associated genetic change?
Denys-Drash: Wilms, renal Dz (proteinuria during infancy, nephritic syndrome, progressive renal failure), male pseudohermaphroditism
Associated genetic change: point mutation of WT1 gene
What is Beckwith-Wiedemann syndrome, and what is the associated genetic change?
Beckwith-Wiedemann: macrosomia, macroglossia, omphalocele, hemihypertrophy
Associated genetic change: 11p15.5, duplication of WT2 locus
What transcription factor is important for normal kidney/gonadal development and is associated with Wilms?
WT1 (a zinc finger protein) is associated with Wilms and is important for normal kidney/gonadal development.
What is the function of WT2?
Function of WT2 is unknown. It affects IGF2, the H19 tumor suppressor, and p57 cell cycle protein.
What are the other genetic defects seen in Wilms?
LOH 1p + 16q, FWT1 (17q), and FWT2 (19q)
Name 1 paternal and 1 maternal environmental risk factor for WT.
Fathers who are welders/machinists (RR 5.3); mothers who use hair dyes (RR 3.6)
What are some poor prognostic factors seen in Wilms?
Unfavorable histology (UH), advanced tumor stage, molecular (+telomerase) and genetic (LOH 1p + 16q) markers, age >24 mos
What histology has the worst outcome in Wilms?
Diffuse anaplasia (DA), followed by rhabdoid and clear cell sarcoma. A review of NWTS-1 and -2 studies involving ∼1,200 children, DA had the shortest survival time compared to non-anaplastic histologies (Bonadio F et al., JCO 1985). In another study, DA was seen in 10% of cases, but accounted for 60% of the deaths (Faria P et al., Am J Surg Pathol 1996).
What study demonstrated the prognostic importance of LOH 1p + 16q for Wilms?
NWTS-5 analysis (Grundy PE et al., JCO 2005 ). For favorable histology (FH), LOH 1p or 16q is associated with ↑ (RR) of relapse. LOH of both ↑ RR of relapse + death.
What are the UH subtypes in Wilms?
Anaplastic: focal or diffuse
How is focal anaplasia defined?
Focal anaplasia is sharply localized within the primary tumor, without atypia in the rest of the tumor.
What renal tumors are not Wilms tumor but are treated similarly to Wilms tumors?
Malignant rhabdoid tumor and clear cell sarcoma of the kidney
What are the 4 sets of criteria used to define DA?
Criteria to define DA:
1. Nonlocalized
2. Localized with severe nuclear unrest elsewhere in the tumor
3. Anaplasia outside the tumor capsule or mets
4. Anaplasia revealed by random Bx
What is the stage-by-stage 4-yr OS for anaplastic/UH WT?
4-yr OS for anaplastic/UH Wilms:
Stage I: 83%
Stage II: 83%
Stage III: 65%
Stage IV: 33%
(Dome JS et al., JCO 2006)
How does the 4-yr OS compare between focal and diffuse anaplasia?
Overall: 97% vs. 50%
Stage I: 100%
Stage II: 93% vs. 55%
Stage III: 90% vs. 45%
Stage IV: 80% vs. 4%
What are the typical presenting Sx in Wilms? How does this compare to NB?
Asymptomatic abdominal mass (83%) → abdominal pain (37%), HTN (25%, due to ↑ renin), hematuria (25%), fever, anemia (due to ↓ erythropoietin)
NB most commonly presents with systemic Sx.
(Mnemonic: WWNN—Wilms are Well, Neuroblastomas are Not well)
 WORKUP/STAGING
WORKUP/STAGING
What is the typical workup for an abdominal mass of unclear etiology in a child?
Abdominal mass workup: H&P (focusing on congenital defects), labs, UA (including urinary catecholamines), abdominal US, CXR, and CT C/A/P
What is the recommended 1st-line imaging modality for an abdominal mass?
US is the recommended 1st-line study for imaging the abdomen.
Pts with what histologic subtype(s) require bone scan?
Clear cell
With a Dx of Wilms, what 2 chest imaging modalities can be employed for staging purposes?
Both CXR and CT are used for chest imaging. Lesions seen on CT but not visible on CXR may be treated more conservatively than lung mets visible on CXR.
Pediatric pts with what renal tumors need BM Bx?
Pts with clear cell and rhabdoid require BM Bx.
Pediatric pts with what renal tumors require MRI of the head as part of their workup?
Rhabdoid: 10%–15% will have PNET in brain (atypical teratoid rhabdoid tumors)
Clear cell: to r/o brain mets
What is the typical appearance of WT on CT?
Large round mass with pseudocapsule usually without calcifications.
Under what circumstances should Bx be performed?
Do not Bx unless the tumor is unresectable or bilat Dz. If Bx is necessary, use a posterior approach to avoid contaminating the abdomen.
On what issues should the surgeon comment at the time of surgery?
Involvement of regional nodes, opposite kidney, peritoneum, liver, renal vein/IVC. Also, if there is tumor spillage and if it is confined to the ipsi flank.
What% of patients present with each of the features summarized in this table?
| PresentingFeatures | Patients (%) |
| Bilat Dz | 7 |
| Multifocal Dz | 12 |
| Renal vein invasion | 10 |
| LN involvement | 20 |
| Mets | 10 |
What are some common sites of mets?
Lung (80%) → liver → bone, brain (clear cell), LN (outside abdomen and pelvis)
How commonly is calcification seen in Wilms?
Calcification is seen in 10%–15% of cases but is seen in 85% of NB cases.
How many stages are there in Wilms?
There are 5 stages in Wilms.
Summarize the staging of WT.
I (40% of pts): limited to kidney
II (20%): extension to outside capsule, vessel involvement >2 mm
III (20%): R1-R2 resection, +LN, local spillage or diffuse peritoneal spillage, Bx (including FNA), +implants, +margin, transected tumor thrombus, piecemeal resection, unresectable tumor
IV (10%): hematogenous mets or LN+ outside the abdomen/pelvis
V (4%–8%): bilat Dz; each side staged independently
Is adrenal involvement considered a met?
No. Adrenal involvement is considered local extension.
 TREATMENT/PROGNOSIS
TREATMENT/PROGNOSIS
What is the Tx paradigm for WT in the U.S.?
WT Tx paradigm: initial surgical resection → risk-adapted adj chemo +/– RT
What is the major difference between the International Society of Pediatric Oncology (SIOP) Tx paradigm (European Cooperative Group) and the National Wilms Tumor Study (NWTS) paradigm (American Cooperative Group)?
SIOP trials incorporate preop therapy (CRT), whereas the NWTS/COG trials do not.
Under what circumstance is the SIOP paradigm favored in the U.S.?
In unresectable or bilat Wilms, preop chemo is used.
What are the indications for postop RT in the current COG protocols (AREN0532,533)?
Indications for postop RT depend on histology and stage:
Favorable histology: stages III–IV
Unfavorable histology: stages I–IV
What chemotherapeutic agents are typically used in Wilms?
Vincristine, actinomycin D (Adr/VP-16/Cytoxan/carboplatin added in UH)
What did the early NWTS-1 and NWTS-2 studies show?
1. Vincristine and actinomycin D (VA) are better together than either alone.
2. RT is not needed for stage I FH pts, but when given it should preferably start within 9 days of surgery (but no later than postop day 14).
3. There was no RT dose response from 10–40 Gy.
Which study demonstrated that whole abdomen irradiation (WAI) is not needed for local spillage?
NWTS-1; flank fields suffice if spillage is local.
Which study demonstrated that adding Adr to VA benefited group 2–4 pts?
NWTS-2; adding Adr benefited group 2–4 FH, especially group 2–4 UH pts (OS 38% vs. 78%).
Which study demonstrated that 10 wks was equal to 6 mos of chemo for stage I pts?
NWTS-3; 4-yr OS was 96%–97%.
Which study showed that stage II FH pts do not need RT as long as VA is given?
NWTS-3 (4-arm: vincristine/Actinomycin D/Adriamycin [VAAdr] vs. VA vs. +/– RT → 4-yr OS ∼90%–95%, no difference)
Which study eliminated Adr from stage II FH?
NWTS-3. VA alone was sufficient.
Which study demonstrated that 10 Gy was equal to 20 Gy if Adr was added to stage III pts?
NWTS-3 demonstrated the noninferiority of lower RT doses with Adr.
Which study addressed the addition of Cytoxan to VAAdr for high-risk pts?
NWTS-3. Cytoxan improved outcome in UH stage II–IV but not FH stage IV.
Which study addressed pulse-intense (PI) chemo?
NWTS-4. 6 mos of PI was equal to 15 mos of conventional chemo.
What are the main advantages of PI chemo?
With PI chemo, there is ↓ hematologic toxicity and ↓ total cost b/c fewer drugs are used.
Which study found that local spillage (old stage II) without RT results in a ↑ LR?
NWTS-4; ↑ LR, but no difference in OS; so, moved to stage III for FH (need adj RT)
What question does NWTS-5 address? (Dome JS et al., JCO 2006)
Nonrandomized, assesses prognostic importance of LOH 1p + 16q
For which pts did NWTS-5 show ↑ (13.5%) rates of relapse with nephrectomy alone and without adj chemo?
Stage I FH, pts <2 yo, and tumors <550 g. Most (>70%) were salvaged successfully, however.
What chemo regimen in NWTS-5 improved outcomes for stages II–IV with DA?
Vincristine/Adr/cyclophosphamide/etoposide
Did stage I anaplastic tumors qualify for RT in NWTS-5?
No. Anaplastic tumors did not qualify for RT in NWTS-5.
What do the current protocols (COG AREN0532, 0533) address?
Tx intensification based on LOH 1p16q status; stage I anaplastic pts get RT + Adr (with VA).
What were the factors that determine risk groups in the COG AREN0532/0533?
Age (>2 yo worse), tumor weight (550 g), stage, LOH 1p + 16q, and chemo response
What subset of pts on the current COG protocol could get surgery alone without adj Tx?
Very low risk group (stage I FH, pts <2 yo, and tumors <550 g) and if there is central pathology review and LN sampling
What are the RT doses to the postop bed for Wilms pts ≥16 yo and/or those with rhabdoid and/or DA? How about for other pts?
19.8 Gy to flank for stage III DA or rhabdoid stages I–III (+10.8 Gy boost to mets/gross Dz = 30.6 Gy), 10.8 Gy for the rest (stage III FH, stages I–III FA, stages I–II DA, stages I–III clear cell, age <16 yrs, infants with DA or rhabdoid histology)
What are the indications and the RT doses for WAI?
Seeding/rupture/diffuse spill; 10.5 Gy (1.5 Gy/fx), boost to 21 if bulky (but 19.8 Gy for DA or rhabdoid)
What are the indications for flank RT?
Stage III FH, localized spill, stages I–III UH, and recurrent Wilms (also done for certain stage IV pts)
What is the standard flank RT dose?
The standard flank RT dose is 10.8 Gy in 6 fractions.
What is the dose to unresected +LNs?
19.8 Gy to entire chain → boost with optional 5.4–10.8 Gy; 30.6 Gy if >16 yo
What is the preferred Tx for localized liver mets? Diffuse liver mets?
Surgery is preferred for localized liver mets. For diffuse liver mets, 19.8 Gy to the entire liver (with optional boost of 5.4–10.8 Gy) is an option.
What dose is given to resected +LNs?
Resected +LNs get a dose of 10.8 Gy.
At what age can pts rcv greater flank doses and greater doses to mets?
≥16 yo (19.8 Gy to flank or WAI and 30.6 Gy to mets in bone, LNs, and brain)
When is whole lung irradiation (WLI) not required in a Wilms pt with lung mets?
WLI is not required in these pts if mets are seen only on CT and not on CXR or if a CR is seen after VAAdr at wk 6.
When is WLI indicated? What are the doses?
WLI is indicated when there is no CR seen on CT at wk 6 after 3-drug chemo (per current protocol); it is not based on # of mets, size, or detectability on CT or CXR. The dose for WLI is 12 Gy (>1 yo) or 10.5 Gy (<1 yo) in 1.5 Gy/fx. If there is persistent Dz after WLI, consider a 7.5 Gy boost.
What med should pts take when treated with WLI?
Trimethoprim/sulfamethoxazole (Bactrim) for PCP prophylaxis
How is bilat Wilms treated?
Initial surgery or Bx to stage each side → chemo → 2nd-look surgery at 6 wks for a max safe resection (spare two-thirds of 1 kidney if possible) → continuation of chemo. RT is given after surgery based on the final local stage.
RT should preferably start by which day and should begin no later than which day after surgery?
RT should preferably start by day 9 and should begin no later than day 14. Secondary analyses of NWTS-1 and NWTS-2 showed worse outcomes when RT was delayed >10 days.
How long is the chemo regimen for stages I–II and III–IV FH?
18 wks (VA); 24 wks (VAAdr)
What is the medial border of a flank field?
1 cm from the contralat vertebral body edge. Be aware of the intact kidney location.
What are the preferred RT margins/techniques for a flank field?
Preop GTV + 1 cm; AP/PA for flank; conformal for boost (residual + 2 cm)
What is the dose for brain mets?
The dose for brain mets is WBRT to 21.6 Gy if <16 yo (+ 10.8 Gy boost = 32.4 Gy) or 30.6 Gy (–boost) if >16 yo.
What is the dose for bone mets?
The dose for bone mets is 25.2 Gy (30.6 Gy if >16 yo).
How do you manage a pt who presents with mets and a resectable tumor?
These pts are treated the same way as nonmetastatic pts, except mets are treated at the same time as abdominal RT, if needed.
What is the outcome for relapsed Wilms treated with VA only for stage I or II Dz?
4-yr EFS/OS: 71% (stage I) vs. 82% (stage II). Pt salvaged with surgery, RT, and chemo with vincristine/Adr/Cytoxan/etoposide. Lung mets only, 4-yr EFS/OS: 68% (stage I) vs. 81% (stage II).
What about relapsed stages III–IV Dz?
Relapse after stages III–IV Tx is worse (4-yr EFS/OS: 42% vs. 48%, respectively), lung only mets: 4-yr EFS/OS: 49% vs. 53%, respectively. (Green DM et al., Ped Blood Cancer 2007; Malogolowkin M et al., Ped Blood Cancer 2008)
 TOXICITY
TOXICITY
What is the dose constraint for the kidney?
One-third of contralat kidney <14.4 Gy
What is the dose constraint for the liver?
One-half of uninvolved liver <19.8 Gy; with liver mets, 75% of liver ≤30.6 Gy
Pts are at risk for what late effects with flank RT? WLI?
Scoliosis of the spine, muscular hypoplasia, kyphosis, iliac wing hypoplasia, SBO, veno-occlusive Dz of the liver;
Breast hypoplasia (four-fifths of females who get WLI will have underdeveloped breasts), pneumonitis, CHF, 2nd malignancy, and renal failure
What is the risk of SBO at 15 yrs after flank/abdominal RT?
15%.
What is the risk of a 2nd malignancy at 15 yrs?
1.6%–2%.
The reirradiation tolerance of which organ decreases with time after initial RT?
Reirradiation tolerance of the kidney decreases with time.
What is the TD 5/5 for an entire kidney?
The TD 5/5 is 23 Gy.
What is the cumulative maximal total dose (including prior RT) for WT pts?
30.6 Gy (if <3 yrs) or 39.5 Gy (if >3 yrs)
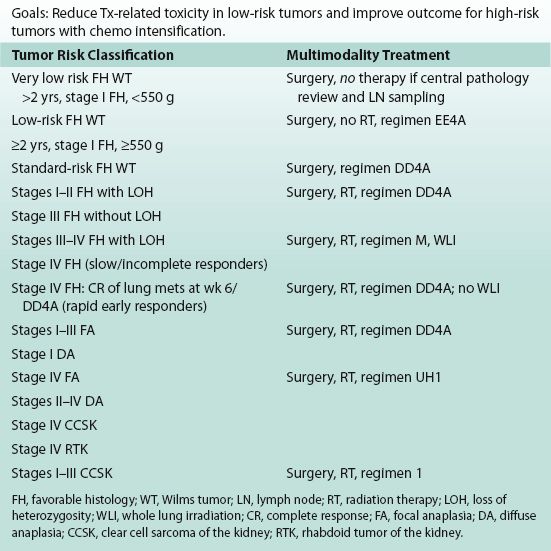
Table 3.1 Current Children’s Oncology Group Wilms Protocol (AREN0532/533)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


