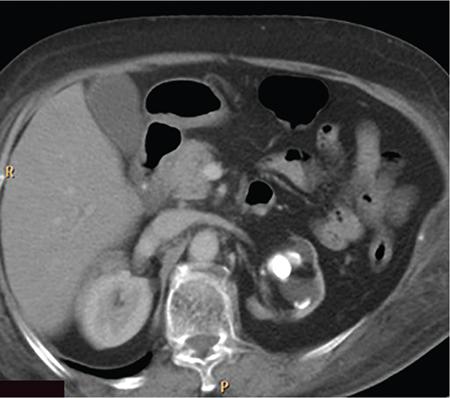
Xanthogranulomatous pyelonephritis (XGP) is a rare, chronic inflammatory condition of the kidneys characterized by renal parenchymal destruction and replacement by lipid laden foamy macrophages. (Xantho means yellow, yellow colour imparted to renal parenchyma and inflammatory masses by abundance of lipid laden macrophages.) It is first described by Schlagenhaufer in 1916. Aetiology is often unclear, however considered multifactorial, mostly as a combination of renal obstruction and recurrent infection/inflammation. Recurrent bacterial infections along with an incomplete immune response to organisms such as Proteus mirabilis, E. coli along with multiple other bacteria are implicated. The disease is most commonly seen in women of middle age group, however elderly and children are also affected. Most commonly, seen to be associated with an obstructive renal calculus, however destruction of the renal parenchyma is due to severe inflammation than obstruction. There is also an increased incidence of diabetes mellitus and other metabolic diseases among the patients. Lymphatic obstruction, malnutrition, arterial insufficiency, venous occlusion and haemorrhage are other factors implicated. In addition, it has been presented as a complication of renal transplant. Various predisposing factors are summarized in the following box. It can occur at any age, but most frequently in the fifth to sixth decades. Female predilection is seen likely due to higher incidence of UTIs and thus struvite (staghorn) calculi. There is also an increased incidence in patients with diabetes mellitus. Most of the cases are associated with a pelvic renal calculus which assumes a staghorn shape (struvite calculi). Along with the subsequent hydronephrosis, chronic inflammation and other precipitating factors mentioned above lead to scarred contracted renal pelvis, dilated calyces and diffuse infiltration of the renal parenchyma by plasma cells and lipid laden macrophages, which may form multiple yellow coloured masses. Microscopic examination shows ulcerated calyceal mucosa which is replaced by necrotic debris and inflammatory cells, mainly polymorphonuclear leukocytes. Granulation tissue with multinucleated macrophages will be seen in the adjacent tissue. The inflammatory zone is associated with plasma cellular infiltrate and bordered by a band of fibrous tissue. Macroscopically and in radiological studies, infiltration of perirenal tissues, psoas muscle, adjacent small bowel, diaphragm and soft tissues are often seen. Involvement of ureter has also been reported. Two main types of XGP are described focal (10%–17%) and diffuse (80%). Focal XGP imitates a renal mass and hence has been described as ‘Great imitator’ main differential being Wilms’ tumour. Focal form of XGP is usually seen in the renal cortex, with no communication with pelvis. An obstructive renal calculus may not be always present. As it often mimic a renal tumour, it is hence considered a pseudotumour. The diffuse type affects the whole kidney and is more common in children. A third, segmental form has also been mentioned. Staging for XGP is proposed by Malek and Elder. There are three stages. Symptoms are highly variable with patients presenting with acute symptoms such as fever, flank pain, UTI similar to pyelonephritis or chronic nonspecific symptoms such as weight loss, malaise and anorexia. On physical examination, a palpable mass in the flank along with tenderness can be elicited. A draining renal cutaneous fistula is seen in 5% of patients. Sometimes the patient can be asymptomatic as well. Lab parameters will show anaemia, raised erythrocyte sedimentation ratio, leukocytosis. Urine analysis may show positive urine culture, microscopic haematuria, proteinuria and pyuria.. Most often urinary tract symptoms are absent, in such cases pyuria and positive urine cultures (95% and 60%, respectively) are present. XGP can also present as a complication of renal transplant and diabetes mellitus. The above-mentioned macroscopic forms (focal and diffuse) are recognized on imaging. Diffuse form accounts for 90% of the cases. Focal form also known as tumefactive form constitutes approximately 10% of cases and sometimes can represent diffuse XGP of one moiety of a duplex system. Cross-sectional imaging is the most important modality for diagnosis as findings in plain radiograph or intravenous urography (IVU) alone is nonspecific. However, ultrasound is the first modality of imaging since it helps in differentiating focal from diffuse form. However, no radiologic features are characteristic of XGP. Diagnosis with plain radiography is not always possible. The main differentials include a cute pyelonephritis, renal cell carcinoma and renal calculus disease and differentiating between them is difficult. Staghorn calculi will be seen most often (75% of cases) in XGP. Renal outline may appear enlarged and fragmented. Perinephric extension of inflammation will produce an ill-defined renal margin. The kidneys will be nonfunctioning on the affected side with no excretion (absent nephrogram seen). Sometimes a partially enhancing and excreting kidneys can be seen. Similar findings are seen in chronic hydronephrosis with associated cortical thinning. Focal lesions show no function or a patchy nephrogram. Associated splaying and stretching of the calyces can be seen. It is commonly the first imaging modality. Ultrasonography findings usually demonstrate an enlarged kidney with loss of corticomedullary differentiation and maintained reniform shape. The renal pelvis is small due to fibrosis. Calyces will appear dilated with an echogenic rim. Cortical thinning occurs with replacement of renal parenchyma by hypoechoic masses which represent hydrocalyces, small abscesses or granulomas. As these hypoechoic areas are not simple fluid-filled spaces, they may not show posterior acoustic enhancement and thus differentiating from simple hydronephrosis, latter will show dilated calyces which are sharply defined and demonstrate post acoustic enhancement. A staghorn calculus will be usually demonstrated, may or may not show posterior acoustic shadowing. Ultrasonography can easily differentiate diffuse form from focal form. There is generalized enlargement of kidneys with focal hypoechoic areas described above, in case if diffuse XGP. Whereas the focal form may appear as a focal heterogeneous mass, which can be often misdiagnosed as a tumour. The main disadvantage of ultrasonography is that it is less sensitive than other modalities in demonstrating extrarenal spread. Also, similar appearances are also seen in simple hydronephrosis associated with renal calculus, pyonephrosis, renal TB, cystic neoplasm and lymphoma. CT is the main modality for assessing perirenal extension and is essential for preoperative evaluation. The findings are most helpful in reaching the diagnosis. In diffuse disease, generalized enlarged nonfunctioning kidney with a staghorn calculus will be seen. Calculus is usually located centrally within the pelvis causing obstruction (Fig. 10.12.2.3.1). Although the reniform shape is usually maintained, the parenchyma is usually destroyed and replaced by hypodense masses of low attenuation (–10 to 30 Hounsfield units [HU]). These dilated cavities and abscesses filled with pus and debris give a multilocular appearance that has been described similar to the paw print of a bear. This sign is characteristic of XGP and has been described as ‘bear paw sign’. Perinephric fat stranding and thickening of Gerota’s fascia is often seen. Calcifications in the xanthomatous masses are easily identified in CT scan. Intrarenal cortical abscesses may show small gas collections within. Renal atrophy has also been described rarely.
3. Xanthogranulomatous pyelonephritis
Introduction
Epidemiology
Pathology and staging
Staging system
Stage 1
Nephric stage
Inflammation confined to kidneys
Stage 2
Perinephric stage
Inflammation extends to the perirenal fat.
Stage 3
Inflammation further extends into surrounding retroperitoneum.
Clinical features
Radiographic features
Plain radiography
Intravenous urography
Ultrasound
Computed tomography
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


