Zenker Diverticulum
Michael P. Federle, MD, FACR
Key Facts
Terminology
Mucosal herniation through area of anatomic weakness in region of cricopharyngeal muscle
Imaging
Barium-filled sac posterior to cervical esophagus
Opening into pouch just above cricopharyngeus muscle (C5-6 level)
Prominent or thickened cricopharyngeal muscle
Luminal narrowing at pharyngoesophageal junction due to extrinsic compression
Large diverticulum may protrude laterally to left or compress cervical esophagus
Almost all patients have associated esophageal dysmotility, often with hiatal hernia and GERD
Top Differential Diagnoses
Killian-Jamieson diverticulum
Opening below cricopharyngeus muscle
Protrude laterally
Esophageal webs
Epidermolysis and pemphigoid
Clinical Issues
Upper esophageal dysphagia
Regurgitation and aspiration of undigested food
Complications
Risk of perforation during endoscopy or placement of nasogastric tube
Aspiration pneumonia (in 30% of cases)
Risk of carcinoma (seen in 0.3% of cases)
Surgical diverticulectomy or endoscopic repair
Diagnostic Checklist
Following repair of Zenker diverticulum, residual outpouching will still be seen in most cases
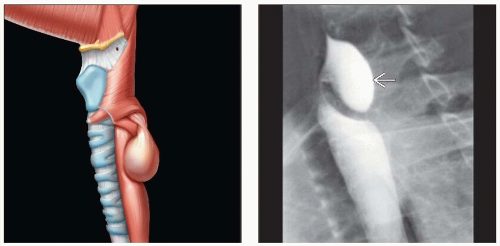 (Left) Graphic shows a pouchlike herniation through the Killian dehiscence in the cricopharyngeal muscle. (Right) Lateral view of a barium swallow shows a large pouch  arising from the posterior pharyngoesophageal junction. arising from the posterior pharyngoesophageal junction. |
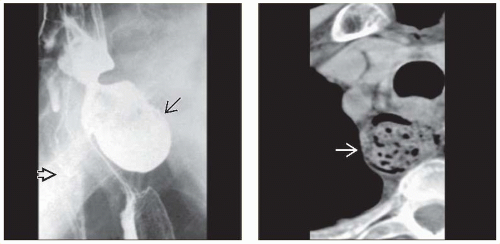 (Left) A film from a barium esophagram shows a large diverticulum  arising from the pharyngoesophageal junction and extending into the mediastinum. The esophagus is displaced, and its lumen is narrowed by the diverticulum. Note the barium aspirated into the trachea arising from the pharyngoesophageal junction and extending into the mediastinum. The esophagus is displaced, and its lumen is narrowed by the diverticulum. Note the barium aspirated into the trachea  . (Right) Axial NECT in the same patient shows the diverticulum . (Right) Axial NECT in the same patient shows the diverticulum  filled with debris, fluid, and gas. Large diverticula often compress the lumen of the esophagus and extend to 1 side of the midline due to mass effect. filled with debris, fluid, and gas. Large diverticula often compress the lumen of the esophagus and extend to 1 side of the midline due to mass effect. |
TERMINOLOGY
Synonyms
Pharyngoesophageal diverticulum or posterior hypopharyngeal diverticulum/outpouching
Definitions
Mucosal herniation through area of anatomic weakness in region of cricopharyngeal muscle
IMAGING
General Features
Best diagnostic clue
Barium-filled sac posterior to cervical esophagus
Location
Killian dehiscence (triangular anatomical area of weakness)
Midline posterior wall of pharyngoesophageal segment just above cricopharyngeus muscle (C5-6 level)
Between oblique and horizontal fibers of cricopharyngeal muscle (most common site) or between thyro-/cricopharyngeal muscles
This area of weakness occurs in 1/3 of patients
Size
Average maximal dimension: 2.5 cm
Range: 0.5-8 cm
Morphology
Posterior hypopharyngeal saccular outpouching with neck opening above cricopharyngeus muscle
Zenker diverticulum is a false diverticulum
Presence of mucosa and submucosa
Lack of muscle
Almost all patients have associated esophageal dysmotility, often with hiatal hernia and gastroesophageal reflux disease (GERD)
On barium studies: Any irregularity of contour of Zenker diverticulum suggests either inflammatory or neoplastic complication
Radiographic Findings
Radiography
Chest x-ray
May show air-fluid level in superior mediastinum
Fluoroscopic-guided barium study
Frontal view
Barium-filled sac below level of hypopharynx
Large diverticulum: Extends inferiorly into mediastinum
Lateral or oblique view
Barium-filled sac posterior to cervical esophagus
Neck of diverticulum with its opening into posterior hypopharyngeal wall above cricopharyngeus muscle
Prominent or thickened cricopharyngeal muscle
Luminal narrowing at pharyngoesophageal junction due to extrinsic compression
Persists after passage of bolus through esophagus
± nasopharyngeal regurgitation
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree