Merkel Cell Carcinoma, Skin
Nayela Keen, MD
Christine M. Glastonbury, MBBS
Key Facts
Terminology
Neuroendocrine skin malignancy derived from Merkel cells
Rare but aggressive, rapidly growing cutaneous malignancy
Imaging
Primary tumor variable but may be small or not discernible on clinical exam
Imaging important for assessing nodes
CT or MR: Useful for assessing nodal spread
MR may be more sensitive for intralymphatic spread and deep extent of tumor
PET: High FDG avidity makes ideal staging agent
Top Differential Diagnoses
Skin basal cell carcinoma
Skin SCCa
Skin melanoma
Pathology
Associated with sun exposure
Merkel cell polyomavirus associated with most
Immunocompromised patients have higher incidence, often present in later stage and worse prognosis
MCC AJCC staging system introduced in 2010
Clinical Issues
Most patients > 65 years
Painless, firm, red nodule that grows rapidly
Early and frequent metastasis to regional lymph nodes
Nodal metastasis most important predictor of outcome
Wide local excision is important; XRT has role
2x the mortality rate of melanoma
5-year relative survival if N0 at diagnosis ˜ 75%, if nodal mets ˜ 45%
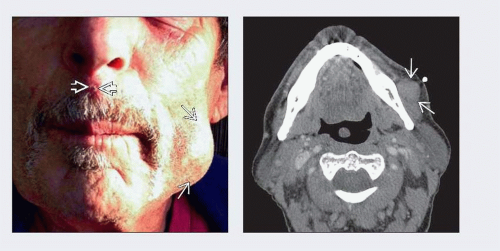 (Left) Clinical photograph demonstrates subtle, small lesion of midline face, just above the upper lip  , which at biopsy proved to be Merkel cell carcinoma. Also notice marked fullness of left lower cheek , which at biopsy proved to be Merkel cell carcinoma. Also notice marked fullness of left lower cheek  . (Right) Axial CECT in same patient with skin marker demonstrates enlarged left facial node . (Right) Axial CECT in same patient with skin marker demonstrates enlarged left facial node  without necrosis or calcifications. This corresponds to lower left cheek palpable and visible mass. Additional small bilateral submandibular nodes were also evident on this CECT. without necrosis or calcifications. This corresponds to lower left cheek palpable and visible mass. Additional small bilateral submandibular nodes were also evident on this CECT. |
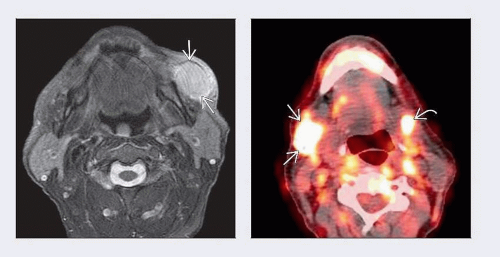 (Left) Axial T2WI FS MR in same patient obtained almost 4 weeks after initial CT shows marked increase in size of left facial node  without necrosis. Case well illustrates the potential for rapid growth of Merkel cell carcinoma. (Right) Axial fused PET/CT obtained 1 week prior to MR shows avid FDG uptake in small left submandibular node without necrosis. Case well illustrates the potential for rapid growth of Merkel cell carcinoma. (Right) Axial fused PET/CT obtained 1 week prior to MR shows avid FDG uptake in small left submandibular node  and large right IB node and large right IB node  . Larger left facial node shown on CT above and MR to left was also markedly FDG avid (SUV = 15). . Larger left facial node shown on CT above and MR to left was also markedly FDG avid (SUV = 15). |
TERMINOLOGY
Abbreviations
Merkel cell carcinoma (MCC)
Synonyms
Neuroendocrine carcinoma of skin
Definitions
Neuroendocrine skin malignancy derived from Merkel cells
Part of the mechanoreceptor complex in skin
Located at basal layer of epidermis
Probably derived from neural crest cells
IMAGING
General Features
Best diagnostic clue
Nodal mass within neck associated with possible focal skin thickening
Primary site may be subtle clinically as well as radiographically
Location
Most commonly arises on facial skin
50% of cases occur in head and neck
Cheeks, nose, perioral, eyelids, periocular
30% occur on extremities
5-7% occur on trunk
< 15% unknown primary site
Even more rarely arises from mucosal surfaces
Size
Median diameter of primary at diagnosis = 1.1 cm
May present from adenopathy without discernible primary
Morphology
If primary visible, appears as exophytic subcutaneous nodule
CT Findings
CECT
Primary: Skin thickening or subcutaneous mass
Solid nodal disease, moderately enhancing
MR Findings
Primary site is typically small and may not be evident on imaging
If lesion seen, typically T2 hyperintense and moderately to markedly enhances with contrast
May see abnormal adjacent nodularity or hyperintensity of subcutaneous fat to suggest intralymphatic spread
Involved nodes of variable size, typically solid and moderately enhance with contrast
Nuclear Medicine Findings
PET/CT
Merkel cell carcinoma is highly FDG avid
Useful for staging, surveillance, restaging recurrent disease and distant metastasis
Even small nodes may show increased FDG uptake
Lymphoscintigraphy may be used to locate sentinel nodes
Increasingly important role in MCC treatment
Imaging Recommendations
Best imaging tool
MR most accurate evaluation of primary tumor extentRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


