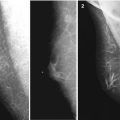
Fig. 9.1
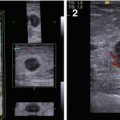
The status after radical resection of the breast in a man. Local recurrence of breast carcinoma. (a) Photo. (b) (1–5) Grayscale US, panoramic scan, PDI, 3D, ARFI, and US elastography
Solid lesion
Size of 1–2 cm
Decreased echodensity
Homogeneous structure
Irregular or roundish shape
Rough borders
Indistinct contours
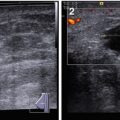
Intranodular blood flow pattern in color Doppler imaging (CDI), power Doppler imaging (PDI), and three-dimensional power Doppler vascular image reconstruction (3DPD)
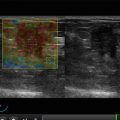
Intensive hard (blue) staining with US elastography
Average shear-wave velocity with acoustic radiation force impulse (ARFI) of 2.9 m/s
Strain ratio of 2.6
Any surgical intervention may be accompanied by oleogranuloma or adipose necrosis in the late postoperative period (3–6 months and later after surgery). Lipogranuloma can be detected along the postoperative scars as a lesion of various echodensity (anechoic, hypoechoic, or hyperechoic) and size (more often <10 mm) of roundish shape with clear margins, homogeneous (or impure) echostructure, and avascular with CDI, PDI, and 3DPD. It is often accompanied with acoustic shadow, especially in cases of calcifications, which are characteristic for lipogranuloma. Surrounding tissues are usually intact or exhibit the signs of lymphostasis. Adipose necrosis and lipogranuloma are difficult to differentiate from recurrent breast carcinoma. Recurrent tumors of small sizes can have the same echodensity, echostructure, shape, contours, and vascularity.
Local fibrosis (Fig. 8.3) is characterized by decreased echodensity (100 %) and layered structure (93 %) and lipogranuloma with average or mixed echodensity (29 and 45 %, respectively), heterogeneous structure (97 %), small calcified incorporations (68 %), “eggshell” calcification (32 %), and fluid component (29 %). Acoustic shadows can be observed significantly more often in patients with lipogranulomas (87 %) than in recurrent tumors (2 %). Posterior enhancement of US does not depend on the type of the mentioned lesions. Lipogranulomas, local fibrosis, and cystic lesions are usually avascular, whereas recurrent breast carcinoma is vascularized in CDI, PDI, and 3DPD in 83 % of cases.
US and X-ray mammography are always used together to diagnose local recurrence of breast carcinoma. However, US is unique, widely accessible, and cost-effective as an imaging technique for recurrences in the region of a radical mastectomy (Sencha et al. 2011a, b). The sensitivity of US in the diagnosis of recurrent breast carcinoma in the region of radical resection is 91–93 %; the specificity, 96 %; and the diagnostic accuracy, 93–94 %. The corresponding figures for X-ray mammography are 87, 84, and 86 % (Sinyukova and Sholokhov 2010). Puncture biopsy of solid masses in the postoperative scar and the bed of the operated breast is obligatory to verify the lesion’s nature. Oncologic awareness of female population and general practitioners associated with mammographic and US screening can lead to the early diagnosis of breast tumors, increase the life expectancy of patients, and improve life quality.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


