Neoplastic |
Metastatic tumor
Fig. 1.94a, b
Fig. 1.95 |
Single or multiple well-circumscribed or poorly defined lesions involving the skull, dura, leptomeninges, and/or choroid plexus; low to intermediate attenuation, usually with contrast enhancement, with or without bone destruction, with or without compression of neural tissue or vessels. Leptomeningeal tumor often best seen on postcontrast images. |
Metastatic tumor may have variable destructive or infiltrative changes involving single or multiple sites of involvement. |
Schwannoma (neurinoma): acoustic, trigeminal, etc.
Fig. 1.96
Fig. 1.97a, b |
Circumscribed or lobulated extra-axial lesions, low to intermediate attenuation, with contrast enhancement. Attenuation and contrast enhancement can be heterogeneous in large lesions. |
Acoustic (vestibular nerve) schwannomas account for 90% of intracranial schwannomas and represent 75% of lesions in the cerebellopontine angle cisterns; trigeminal schwannomas are the next most common intracranial schwannomas, followed by facial nerve schwannomas and multiple schwannomas seen with neurofibromatosis type 2. |
Meningioma
Fig. 1.98a, b
Fig. 1.99a, b |
Extra-axial dural-based lesions, well-circumscribed; supra- > infratentorial; intermediate attenuation signal, usually with contrast enhancement, with or without calcifications. |
Most common extra-axial tumors, usually benign neoplasms, typically occur in adults (older than 40 y), women > men; multiple meningiomas seen with neurofibromatosis type 2; can result in compression of adjacent brain parenchyma, encasement of arteries, and compression of dural venous sinuses; rarely invasive/malignant types. |
Hemangiopericytoma |
Extra-axial mass lesions, often well circumscribed; intermediate attenuation, with contrast enhancement (may resemble meningiomas), with or without associated erosive bone changes. |
Rare neoplasms in young adults (men > women) sometimes referred to as angioblastic meningioma or meningeal hemangiopericytoma; arise from vascular cells/pericytes; frequency of metastases > meningiomas. |
Paraganglioma glomus jugulare
Fig. 1.100a–c |
Extra-axial mass lesions located in jugular foramen, often well circumscribed; intermediate attenuation, with contrast enhancement; often associated with erosive bone changes and expansion of jugular foramen. |
Lesions, also referred to as chemodectomas, arise from paraganglia in multiple sites in the body and are named accordingly (glomus jugular, tympanicum, vagale, etc.). |
Choroid plexus papilloma or carcinoma
Fig. 1.101a, b
Fig. 1.102a, b |
Circumscribed and/or lobulated lesions with papillary projections, intermediate attenuation, usually prominent contrast enhancement, with or without calcifications. Locations: atrium of lateral ventricle (children) > fourth ventricle (adults), rarely other locations such as third ventricle. Associated with hydrocephalus. |
Rare intracranial neoplasms. CT features of choroid plexus carcinoma and papilloma may overlap; both histologic types can disseminate along CSF pathways. Carcinomas tend to be larger, have greater degrees of mixed/heterogeneous attenuation than papillomas. Carcinomas often show invasion of adjacent brain, whereas papillomas often do not. |
Lymphoma |
Single or multiple well-circumscribed or poorly defined lesions involving the skull, dura, and/or leptomeninges; low to intermediate attenuation usually with contrast enhancement, with or without bone destruction. Leptomeningeal tumor often best seen on postcontrast images. |
Extra-axial lymphoma may have variable destructive or infiltrative changes involving single or multiple sites of involvement. |
Neurocutaneous melanosis |
Extra- or intra-axial lesions usually > 3 cm in diameter with irregular margins in the leptomeninges or brain parenchyma/brainstem (anterior temporal lobes, cerebellum, thalami, and inferior frontal lobes); may show no abnormalities on CT, occasionally show zones with intermediate to slightly high attenuation secondary to increased melanin, with or without contrast enhancement. With or without vermian hypoplasia, with or without arachnoid cysts, with or without Dandy-Walker malformation. |
Neuroectodermal dysplasia with proliferation of melanocytes in leptomeninges associated with large and/or numerous cutaneous nevi. May change into CNS melanoma. |
Myeloma/plasmacytoma |
Multiple (myeloma) or single (plasmacytoma) well-circumscribed or poorly defined lesions involving the skull and dura; low to intermediate attenuation, with or without contrast enhancement, with bone destruction. |
Myeloma may have variable destructive or infiltrative changes involving the axial and/or appendicular skeleton. |
Chordoma
Fig. 1.103a–c |
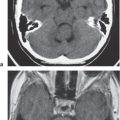
Well-circumscribed lobulated lesions, low to intermediate attenuation, with contrast enhancement (usually heterogeneous); locally invasive associated with bone erosion/destruction, encasement of vessels and nerves; skull base–clivus common location, usually in the midline. |
Rare, slow-growing, malignant cartilaginous tumors derived from notochordal remnants. Detailed anatomical display of extension of chordomas by CT and MRI is important for planning of surgical approaches. |
Chondrosarcoma
Fig. 1.104a, b |
Lobulated lesions, low to intermediate attenuation, with or without chondroid matrix mineralization, with contrast/enhancement (usually heterogeneous); locally invasive associated with bone erosion/destruction, encasement of vessels and nerves; skull base petro-occipital synchondrosis common location, usually off midline. |
Rare, slow-growing tumors. Detailed anatomical display of extension of chondrosarcomas by CT and MRI is important for planning of surgical approaches. |
Osteogenic sarcoma |
Destructive lesions involving the skull base; low to intermediate attenuation, usually with matrix mineralization/ossification, with contrast enhancement (usually heterogeneous). |
Rare lesions involving the skull base and calvarium; more common than chondrosarcomas and Ewing sarcoma; locally invasive; high metastatic potential. Occurs in children as primary tumors and adults (associated with Paget disease, irradiated bone, chronic osteomyelitis, osteoblastoma, giant cell tumor, and fibrous dysplasia). |
Ewing sarcoma |
Destructive lesions involving the skull base; low to intermediate attenuation; usually lack matrix mineralization, with contrast enhancement (usually heterogeneous). |
Rare lesions involving the skull base; usually occur between the ages of 5 and 30 y, males > females; locally invasive; high metastatic potential. |
Sinonasal squamous cell carcinoma |
Destructive lesions in the nasal cavity, paranasal sinuses, and nasopharynx; with or without intracranial extension via bone destruction or perineural spread; intermediate attenuation; mild contrast enhancement; large lesions (with or without necrosis and/or hemorrhage). |
Occurs in adults usually > 55 y, men > women; associated with occupational or other exposure to nickel, chromium, mustard gas, radium, and manufacture of wood products. |
Adenoid cystic carcinoma |
Destructive lesions in the paranasal sinuses, nasal cavity, and nasopharynx, with or without intracranial extension via bone destruction or perineural spread; intermediate attenuation; variable degrees of contrast enhancement. |
Account for 10% of sinonasal tumors; arise from any location within the sinonasal cavities; usually occur in adults older than 30 y. |
Arachnoid cyst
Fig. 1.105a–d |
Well-circumscribed extra-axial lesions with low attenuation equivalent to CSF, no contrast enhancement. Commonly located in the anterior middle cranial fossa > suprasellar/quadrigeminal > frontal convexities > posterior cranial fossa. |
Nonneoplastic congenital, developmental, or acquired extra-axial lesions filled with CSF, usually mild mass effect on adjacent brain; supratentorial > infratentorial locations; men > women; with or without related clinical symptoms |
Lipoma |
Lipomas have CT attenuation similar to subcutaneous fat; typically no contrast enhancement or peripheral edema. |
Benign fatty lesions resulting from congenital malformation often located in or near the midline; may contain calcifications and/or traversing blood vessels. |
Epidermoid cyst
Fig. 1.106a, b |
Well-circumscribed spheroid or multilobulated, extra-axial ectodermal inclusion cystic lesions with low to intermediate attenuation, no contrast enhancement, with or without bone erosion/destruction. Often insinuate along CSF pathways; chronic deformation of adjacent neural tissue (brainstem, brain parenchyma). Commonly located in the posterior cranial fossa (cerebellopontine angle cistern) > parasellar/middle cranial fossa. |
Nonneoplastic congenital or acquired extra-axial off-midline lesions filled with desquamated cells and keratinaceous debris; usually mild mass effect on adjacent brain; infratentorial > supratentorial locations. Adults: men = women, with or without related clinical symptoms. |
Dermoid |
Well-circumscribed spheroid or multilobulated extra-axial lesions with variable low, intermediate, and/or high attenuation, contrast enhancement, with or without fluid/fluid or fluid/debris levels. Can cause chemical meningitis if dermoid cyst ruptures into the subarachnoid space. Commonly located: at or near the midline; supratentorial > infratentorial. |
Nonneoplastic congenital or acquired ectodermal inclusion cystic lesions filled with lipid material, cholesterol, desquamated cells, and keratinaceous debris; usually mild mass effect on adjacent brain. Adults: men slightly > women; with or without related clinical symptoms. |
Fibrous dysplasia
Fig. 1.107 |
Expansile process involving the skull base and calvarium with mixed intermediate attenuation with “ground glass” appearance, heterogeneous contrast enhancement. |
Usually seen in adolescents and young adults; can result in narrowing of neuroforamina with cranial nerve compression, facial deformities, mono- and polyostotic forms (with or without endocrine abnormalities, such as with McCune-Albright syndrome, precocious puberty). |
Paget disease
Fig. 1.108 |
Expansile sclerotic/lytic process involving the skull with mixed intermediate and high attenuation. Irregular/indistinct borders between marrow and inner margins of the outer and inner tables of the skull. |
Usually seen in older adults; can result in narrowing of neuroforamina with cranial nerve compression, basilar impression with or without compression of brainstem. |
Inflammatory |
Subdural/epidural abscess, empyema |
Epidural or subdural collections with low attenuation, thin linear peripheral zones of contrast enhancement. |
Often results from complications related to sinusitis (usually frontal), meningitis, otitis media, ventricular shunts, or surgery. Can be associated with venous sinus thrombosis and venous cerebral or cerebellar infarctions, cerebritis, brain abscess; mortality 30%. |
Leptomeningeal infection/inflammation
Fig. 1.109 |
Single or multiple nodular-enhancing lesions and/or focal or diffuse abnormal subarachnoid enhancement. Leptomeningeal inflammation often best seen on postcontrast images. |
Contrast enhancement in the intracranial subarachnoid space (leptomeninges) usually is associated with significant pathology (inflammation and/or infection vs neoplasm). Inflammation and/or infection of the leptomeninges can result from pyogenic, fungal, or parasitic diseases, as well as tuberculosis. Neurosarcoid results in granulomatous disease in the leptomeninges producing similar patterns of subarachnoid enhancement. |
Eosinophilic granuloma
Fig. 1.110 |
Single or multiple circumscribed soft tissue lesions in the marrow of the skull associated with focal bony destruction/erosion with extension extracranially, intracranially, or both. Lesions usually have low to intermediate attenuation, with contrast enhancement, with or without enhancement of the adjacent dura. |
Single lesion commonly seen in males > females younger than 20 y; proliferation of histiocytes in medullary cavity with localized destruction of bone with extension in adjacent soft tissues. |
|
|
Multiple lesions with syndromes such as Letterer-Siwe disease (lymphadenopathy hepatosplenomegaly), children younger than 2 y; Hand-Schüller-Christian disease (lymphadenopathy, exophthalmos, diabetes insipidus) children 5 to 10 y. |
Sarcoidosis |
Poorly marginated nodular and/or diffuse contrast enhancement in the leptomeninges; may be associated with intra-axial lesions with contrast enhancement, edema, and localized mass effect. |
Multisystem noncaseating granulomatous disease of uncertain cause that can involve the CNS in 5% to 15% of cases. Associated with severe neurologic deficits if untreated. |
Other |
Vascular
AVM
Fig. 1.111a, b |
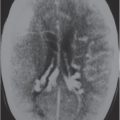
Lesions with irregular margins that can be located in the brain parenchyma, (pia, dura, or both locations). AVMs contain multiple tortuous vessels. The venous portions often show contrast enhancement. Usually not associated with mass effect unless there is recent hemorrhage or venous occlusion. CTA can show the arterial, nidus, and venous portions of the AVMs. |
Supratentorial AVMs occur more frequently (80%–90%) than infratentorial AVMs (10%–20%). Annual risk of hemorrhage. AVMs can be sporadic, congenital, or associated with a history of trauma. |
Dural AVM |
Dural AVMs contain multiple tortuous small vessels at the site of a recanalized thrombosed dural venous sinus. Usually not associated with mass effect unless there is recent hemorrhage or venous occlusion. |
Dural AVMs are usually acquired lesions resulting from thrombosis or occlusion of an intracranial venous sinus with subsequent recanalization resulting in direct arterial to venous sinus communications. Transverse, sigmoid venous sinuses > cavernous sinuses > straight, superior sagittal sinuses. |
Aneurysm
Fig. 1.112a, b |
Saccular aneurysm: Focal, well-circumscribed zone of soft tissue attenuation, with or without wall calcifications; usually shows contrast enhancement.
Fusiform aneurysm: Tubular dilation of the involved artery. |
Abnormal fusiform or focal saccular dilation of the artery secondary to acquired/degenerative etiology, polycystic disease, connective tissue disease, atherosclerosis, trauma, infection (mycotic), oncotic, AVM, vasculitis, and drugs. Focal aneurysms, also referred to as saccular aneurysms, typically occur at arterial bifurcations and are multiple in 20% of cases. The chance of rupture of a saccular aneurysm causing subarachnoid hemorrhage is related to the size of the aneurysm. Saccular aneurysms > 2.5 cm in diameter are referred to as giant aneurysms. Fusiform aneurysms are often related to atherosclerosis or collagen vascular disease. |
Hemorrhagic
Epidural hematoma |
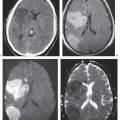
Biconvex extra-axial hematoma located between the skull and dura; displaced dura has high attenuation. The CT attenuation and MRI signal of the hematoma depend on its age, size, hematocrit, and oxygen tension; with or without edema (low attenuation on CT and high signal on T2-weighted images) involving the displaced brain parenchyma; with or without subfalcine, uncal herniation.
Hyperacute hematoma:
CT: Can have high and/or mixed high and intermediate attenuation.
MRI: Intermediate signal on T1-weighted images, intermediate to high signal on T2-weighted images.
Acute hematoma:
CT: Can have high and/or mixed high and intermediate attenuation.
MRI: Low to intermediate signal on T1-weighted images, high signal on T2-weighted images.
Subacute hematoma:
CT: Can have high and/or mixed high and intermediate attenuation.
MRI: High signal on T1- and T2-weighted images. |
Epidural hematomas usually result from trauma/tearing of an epidural artery or dural venous sinus; epidural hematomas do not cross cranial sutures; with or without skull fracture. |
Subdural hematoma |
Crescentic extra-axial hematoma located in the potential space between the inner margin of the dura and the outer margin of the arachnoid membrane. The CT attenuation and MRI signal of the hematoma depend on its age, size, hematocrit, and oxygen tension; with or without edema (low attenuation on CT and high signal on T2-weighted images) involving the displaced brain parenchyma; with or without subfalcine, uncal herniation.
Hyperacute hematoma:
CT: Can have high or mixed high, intermediate, and/or low attenuation.
MRI: Intermediate signal on T1-weighted images, intermediate to high signal on T2-weighted images.
Acute hematoma:
CT: Can have high or mixed high, intermediate, and/or low attenuation.
MRI: Low to intermediate signal on T1-weighted images, low signal on T2-weighted images.
Subacute hematoma:
CT: Can have intermediate attenuation (isodense to brain) and/or low to intermediate attenuation.
MRI: High signal on T1- and T2-weighted images.
Chronic hematoma:
CT: Usually have low attenuation (hypodense to brain).
MRI: Variable, often low to intermediate signal on T1-weighted images, high signal on T2-weighted images, with or without enhancement of collection and organizing neomembrane. Mixed MRI signal can result if rebleeding occurs into chronic collection. |
Subdural hematomas usually result from trauma/stretching/tearing of cortical veins where they enter the subdural space to drain into dural venous sinuses; subdural hematomas do cross sites of cranial sutures; with or without skull fracture. |
Subarachnoid hemorrhage
Fig. 1.67a, b , p. 37 |
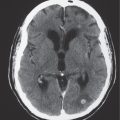
CT: Acute subarachnoid hemorrhage typically appears as poorly defined zones with high attenuation in the leptomeninges within the sulci and basal cisterns. Usually becomes isodense or hypodense after 1 week unless there is rebleeding.
MRI: May not be seen on T1- or T2-weighted images, although it may have intermediate to slightly high signal on FLAIR images. |
Extravasated blood in the subarachnoid space can result from ruptured arterial aneurysms or dural venous sinuses, vascular malformations, hypertensive hemorrhages, trauma, cerebral infarcts, coagulopathy, etc. |