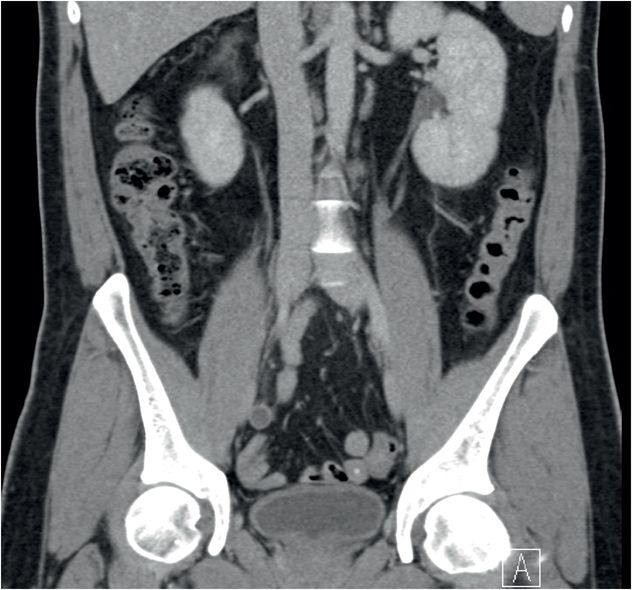
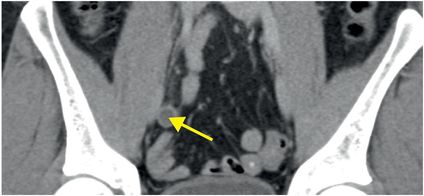
Diagnosis: Appendicitis
Axial (left image) and coronal (right image) contrast-enhanced CT images show a dilated appendix with mild associated fat-stranding (arrows).

Discussion
Overview of appendicitis
Although appendicitis is one of the most common causes of an acute abdomen, clinical diagnosis can be difficult due to the varied presentation and large number of clinical mimics. CT plays a crucial role in diagnosing appendicitis, with an accuracy of 98%.
Appendicitis is thought to be caused by luminal obstruction by an appendicolith (as shown below) or lymphoid hyperplasia, which subsequently causes venous congestion and mural ischemia. The ischemic appendix becomes a nidus for bacterial translocation and inflammation.

The CT diagnosis of appendicitis depends on both direct and indirect imaging characteristics.
Direct signs are due to intrinsic abnormalities of the appendix:
Distended appendix: It is uncommon for the appendix to measure less than 6 mm in a case of appendicitis, although an enlarged appendix in isolation may be a normal variant.
Wall thickening or hyperemia (hyperemia can only be seen on scans with intravenous contrast).
Indirect imaging signs are due to adjacent inflammation:
Periappendiceal fat stranding
Wall thickening of adjacent organs, such as the base of the cecum
Ileus or hydroureter (due to adjacent inflammation)
When evaluating for suspected acute appendicitis, it’s essential to look for potential clinical mimics not related to the appendix, such as pyelonephritis, nephrolithiasis, psoas abscess, and pelvic pathology, all of which can be evaluated by CT.
Clinical synopsis
This patient, a 23-year-old male with early appendicitis, was treated with emergent appendectomy and was discharged without complication the following day.
Self-assessment
|
|
|
|
|
|
|
|
Spectrum of appendicitis
The spectrum of appendicitis ranges from tip appendicitis to inflammation of the entire appendix. Advanced appendicitis may rupture, potentially resulting in abscess formation.
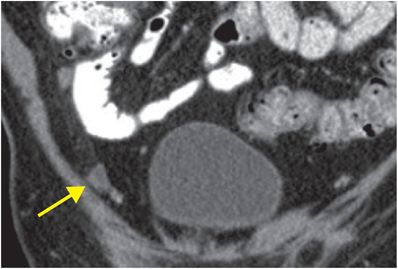
Tip appendicitis
The earliest form of appendicitis can be difficult to detect by CT unless the entire course of the appendix is carefully followed. Occasionally, the entire appendix is normal except for the most distal tip, which is mildly dilated (arrow). The more proximal appendix (inferior to the arrow) is decompressed.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 32 32-year-old male complaining of chest pain after upper endoscopy
32 32-year-old male complaining of chest pain after upper endoscopy
 28 30-year-old male presented with a palpable left testicular mass
28 30-year-old male presented with a palpable left testicular mass
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


