Fracture (traumatic/osteopenic)
Fig. 10.66
Fig. 10.67 |
Traumatic vertebral fracture: Acute/subacute fractures have sharply angulated cortical margins, no destructive changes at cortical margins of fractured end plates; with or without convex outward angulated configuration of compressed vertebral bodies, with or without spinal cord and/or spinal canal compression related to fracture deformity, with or without retropulsed bone fragments into spinal canal, with or without subluxation, with or without kyphosis, with or without epidural hematoma.
Osteopenic vertebral fracture: Acute/subacute fractures usually have sharply angulated cortical margins, no destructive changes at cortical margins of fractured vertebral bodies; with or without compression deformities involving other vertebral bodies, with or without convex outward angulated configuration of compressed vertebral bodies, with or without spinal cord and/or spinal canal compression related to fracture deformity, with or without retropulsed bone fragments into spinal canal, with or without subluxation, with or without kyphosis, with or without epidural hematoma.
Chronic healed fractures usually have normal or near normal signal in compressed vertebral body. Occasionally, persistence of signal abnormalities in vertebral marrow results from instability and abnormal axial loading. |
Vertebral fractures can result from trauma in normal bone or as pathologic fractures in abnormal bone associated with primary bone tumors/lesions, metastatic disease, bone infarcts (steroids, chemotherapy, and radiation treatment), osteoporosis, osteomalacia, metabolic (calcium/phosphate) disorders, vitamin deficiencies, Paget disease, and genetic disorders (osteogenesis imperfecta, etc.). |
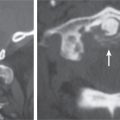
Occipital condyle fractures
Fig. 10.68a–c |
Rough edge fragments of one or both occipital condyles. Fractures may extend to involve the hypoglossal canals and jugular foramina. |
Type 1: Traumatic fracture of condyle with minimal displacement from axial loading mechanism from high-energy blunt trauma (often stable if only unilateral).
Type 2: Fracture of occipital condyle from shear mechanism extending into skull base (can be stable if unilateral or unstable).
Type 3: Transverse fracture of condyle from rotation/bending with injury to alar ligaments that extend from upper lateral portions of the dens to the medial aspects of the occipital condyles. Injury to the alar ligaments results in instability at the occipitocervical junction. |
Atlanto-occipital dislocation |
Abnormal increased distance from the basion of the clivus to the tip of the odontoid using the basion-axial interval (BAI) and/or basion-dental interval (BDI). The BAI is the distance from the basion to a line drawn along the dorsal surface of the C2 body (normal BAI for adults ranges from –4 to 12 mm, children 0 to 12 mm). The BDI is only used in patients older than 13 y and is the distance from the basion to the tip of the dens (normal range 2–12 mm). |
Unstable injury from disruption of ligaments between the occiput, C1, and upper dens from high kinetic energy injuries (usually motor vehicle collisions). Often associated with traumatic injuries to brainstem and cranial nerves. More common in children than adults. |
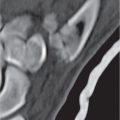
Jefferson C1 fracture
Fig. 10.69 |
Rough edge fractures of the arch of C1, often multiple fracture sites. |
Compression burst fracture of the arch of C1, often stable, can be unstable when there is disruption of transverse or posterior ligament or comminution of anterior arch, often associated with fractures at other cervical vertebrae. |
C2 dens fracture
Fig. 10.70a, b
Fig. 10.71 |
Type I: Fracture at the upper portion of dens above transverse ligament (unstable) from avulsion at the alar ligament.
Type II: Transverse fracture through the lower portion of the dens (may be unstable).
Type III: Oblique fracture involving the dens and body of C2 (usually stable). |
Traumatic fracture involving the upper, middle to lower portions of the dens. |
C2 body fracture type I
Fig. 10.72 |
Fracture of the inferior end plate of C2 with teardrop fragment. |
Extension injury with teardrop fracture of anteroinferior vertebral end plate of the C2 vertebra. |
C2 body fracture type II |
Horizontal fracture plane through the lower body of C2. |
Horizontal shear fracture through the lower portion of the C2 body (lower than C2 dens type III fracture). |
C2 body fracture type III (burst fracture) |
Comminuted fracture of C2 body with or without separation of body from posterior arch (hangman’s fracture). Fracture fragments of C2 body are often displaced peripherally, with or without extension of fragments into spinal canal compression. |
Traumatic comminuted fracture of the C2 body from axial compression force. Often unstable, especially with associated hang-man’s fracture; with or without spinal cord contusion. |
C2 body fracture type IV |
Sagittal plane fracture through C2. |
Severe unstable fracture in the sagittal plane through C2. |
C2 hangman’s fracture
Fig. 10.73a–d |
Disrupted ring of C2 from bilateral pedicle fractures separating the C2 body from the posterior arch of C2. Skull, C1, and C2 bodies are displaced anteriorly with respect to C3. |
Unstable injury from traumatic bilateral pedicle fractures from hyperextension and distraction mechanisms with separation of the C2 body from the posterior arch of C2. Fractures can extend into C2 body and/or through foramen transversarium with injury/occlusion of vertebral artery. Often associated with spinal cord injury. |
Hyperflexion cervical spine injury
Fig. 10.74a, b
Fig. 10.75 |
Sagittal plane fracture associated with compression of the anterior portion of the vertebral body, with teardrop fracture at the anteroinferior portion of the vertebral body or quadrangular fracture extending from the inferior end plate to the anterosuperior cortical margin. A portion of the fractured vertebral body is usually subluxed anteriorly with respect to the vertebral body below with resultant kyphosis. Facet joints are widened due to disruption. Narrowing of the disk height seen below the vertebral body fracture from disk injury. Typically, prevertebral soft tissue swelling is seen, with widened interspinous distance. |
Flexion compression injuries that account for up to 15% of cervical vertebral fractures and often occur from motor vehicle collisions, falls, and diving into shallow water. Fractures involve the anterior portion of the vertebral body with fractures also involving the posterior elements in 50%, with or without tearing of posterior ligaments. Teardrop hyperflexion injuries result in disruption of all ligaments, facet joints, and disks. Quadrangular fractures extend from the inferior to superior cortical margins with disruption of the anterior and posterior longitudinal ligaments and disks. |
Hyperextension injury cervical fracture |
Fractures of vertebral bony arch (laminae, facets, and spinous process) on axial CT images. Sagittal CT images show malalignment of facets and/or spondylolisthesis. |
Extension injury from posterior displacement of the head and upper cervical spine resulting in fractures of the arch (laminae) and/or posterior elements, with or without disruption of anterior longitudinal ligament. Disruption of posterior column results in instability. Can be associated with spinal cord contusion, vertebral artery injury (dissection/occlusion), and other vertebral fractures. |
Hyperflexion-rotation cervical injuries
Fig. 10.76a, b |
Rotatory subluxation of vertebral body and posterior elements, with or without jumped or perched facets, with or without fractures at facets, with or without fracture of the vertebral body. For unilateral locked facet, axial CT image shows rotatory subluxation with absence of normal facet articulation (naked facet sign). Sagittal CT images show perched or jumped facets. |
Hyperflexion-rotation force resulting in traumatic disruption of spinal ligaments (facet-capsular, annular, and/or longitudinal ligaments) with subluxation involving the facet joints with or without fracture. Can occur as unilateral or bilateral locked facets. |
Hyperextension-rotation cervical injuries |
Unilateral fracture of articular pillar, pedicle, and/or lamina, with or without injury/occlusion of vertebral artery. |
Unilateral laminar or facet fracture with ligament disruption (anterior annular and capsular ligaments) from combined hyperextension and rotation mechanism of injury. |
Cervical vertebral burst fracture
Fig. 10.77a, b |
Comminuted fracture extending through both end plates of vertebral body; associated fractures at the posterior elements. |
Comminuted fractures involving the superior and inferior end plates of a cervical vertebral body secondary to axial compression mechanism without fractures involving the posterior elements. Can be unstable if both anterior and middle columns involved. |
Cervical vertebral fracture/dislocation
Fig. 10.78a, b |
Comminuted fractures of posterior elements (laminae, facets, and spinous processes) associated with anterior, lateral, and/or posterior subluxations; with or without fractures involving vertebral bodies, disks, and transverse processes. |
Highly unstable fractures involving all three columns from shear, rotation, and distraction mechanisms. Subluxed fracture components involving the vertebral body usually also involve tearing of the disk. Lateral flexion mechanism of injury resulting in unilateral fracture of articular pillar, with or without fractures of vertebral body, transverse process. |
Cervical lateral flexion injury |
Sagittal plane fracture or articular pillar with malalignment, with or without fracture of vertebral body, transverse process. |
|
Clay shoveler’s fracture |
Avulsion fracture from the spinous processes of C6 and C7. Occasionally occurs at other levels. |
Stable fracture from avulsion of bone from the C6 or C7 spinous processes by the posterior supraspinous ligaments as a result of strong shear forces secondary to lifting heavy weights with arms extended. |
Thoracic/lumbar anterior compression fracture
Fig. 10.79a, b |
Anterior wedge-shaped vertebral body from fractures involving the superior end plate and anterior cortical margin. Multiple fracture lines often seen within the vertebral body. Decrease in height of vertebral body with normal bone density up to 50%. Usually no subluxation because of lack of significant injury to posterior column. |
Flexion-induced fracture of anterior portion of vertebral body from axial load injury involving only the anterior column and sparing the middle and posterior columns. Can occur from trauma in normal or osteoporotic bone. Fractures in the setting of osteoporosis can have delayed or inadequate healing, resulting in progressive height loss. Typically stable because of lack of involvement of the middle and posterior columns. Can involve more than one level. |
Thoracic/lumbar lateral compression fracture |
Lateral wedge-shaped vertebral body from fractures involving the superior end plate and lateral cortical margin. Typically spares the posterior cortical margin of the vertebral body without retropulsed fragments. Commonly occur at T12 to L2 and at T6 and T7; multiple vertebrae involved in 20%. |
Asymmetric fracture involving superior and anterior end plates of vertebral body from asymmetric axial load with or without flexion. Can occur from trauma in normal or osteoporotic bone. Fractures in the setting of osteoporosis can have delayed or inadequate healing resulting in progressive height loss. Typically stable because of lack of involvement of the middle and posterior columns. Can involve more than one level. |
Thoracic/lumbar burst fracture
Fig. 10.80a, b |
Comminuted fracture of vertebral body involving both superior and inferior end plates, decrease in vertebral body height at anterior and posterior cortical margins, often with bone fragments displaced into the spinal canal, widened pedicles; with or without malalignment of fractured vertebral body and/or facets. |
Unstable comminuted compression fractures involving the vertebral body from axial compression mechanism without fractures involving the posterior elements. Can be unstable if both anterior and middle columns involved. |
Thoracic/lumbar facet–lamina fracture |
Fractures involving laminae and facet joints with widened neural arch/pedicles, with or without vertebral body and/or facet subluxation/dislocation, with or without comminution of vertebral body. |
Fractures involving the posterior column from extension, flexion-distraction, or flexion-rotation mechanisms. Often occur between T11 and L4. Unstable fractures occur when all three columns are involved. Can be stable when one or two columns are involved. |
Thoracic/lumbar chance fracture
Fig. 10.81a, b |
Fractures involving the anterior, middle, and posterior columns; anterior wedging of vertebral body with decrease in height of vertebral body often > 50% even with normal bone density. Horizontally oriented fracture planes through vertebral body and posterior elements, disruption/separation of facet joints and interspinous ligaments with widening of the interspinous distance; with or without comminuted fractures of vertebral body, with or without retropulsed fracture fragments from vertebral body into spinal canal; widened interspinous distance; with or without anterior displacement of vertebrae above fracture (distraction fracture). |
Unstable flexion-distraction injury from high-velocity collision or fall causing compression of the anterior column and distraction of middle and posterior columns. Often occurs between T11 and L3. |
Thoracic/lumbar fracture- dislocation |
Comminuted fractures of posterior elements (laminae, facets, and spinous processes) associated with anterior, lateral, and/or posterior subluxations; with or without fractures involving vertebral bodies, disks, transverse processes, and/or ribs. |
Highly unstable fractures involving all three columns from shear, rotation, and distraction mechanisms. Subluxed fracture components involving the vertebral body usually also involve tearing of the disk. |
Fracture/ankylosing spondylitis
Fig. 10.82a, b |
Rigidity of the spine caused by ossification of the anterior and posterior longitudinal ligaments, syndesmophytes, and osteoporosis; increases the predisposition to spinal fractures with minor trauma. Fractures can occur through the vertebral body and/or disk. Also associated with atlantodens instability. |
Autoimmune inflammatory disorder associated with HLA-B27. Inflammation involves the sacroiliac joints, diskovertebral junctions, spinal ligaments, apophyseal joints, costovertebral joints, and atlantoaxial joints. Findings include osteitis, sydesmophytosis, diskovertebral erosions, calcifications along the anterior and posterior longitudinal ligaments, osseous fusion across joints, and osteoporosis. |
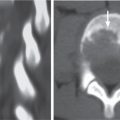
Fracture (malignancy-related)
Fig. 10.83 |
Fractures often associated with destructive changes at cortical margins of vertebrae, with or without convex outward-bowed configuration of compressed vertebral bodies, with or without paravertebral mass lesions, with or without destructive lesions in other vertebrae. |
Neoplasms in bone are associated with bone destruction and decreased capability for maintaining integrity with axial loading, as well as lowering the threshold for fracture with minor trauma. |
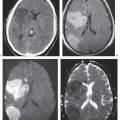
Epidural hematoma |
Epidural collection with low to intermediate and/or slightly high attenuation, with or without spinal cord compression, with or without minimal peripheral pattern of enhancement at hematoma. |
The CT appearance of epidural hematoma depends on the age, hematocrit, and degree of clot formation and retraction. Can be spontaneous or result from trauma or complication (coagulopathy, lumbar puncture, myelography, and surgery). |
Disk herniation
Fig. 10.84 |
Disk herniation/protrusion: Disk herniation in which the head of the protruding disk is equal in size to the neck on sagittal reconstructed images.
Disk herniation/extrusion: Disk herniation in which the head of the disk herniation is larger than the neck on sagittal reconstructed images.
Disk herniation/extruded disk fragment: Disk herniation that is not in contiguity with disk of origin. |
Represents a disk herniation (focal > broad-based) that results from inner annular disruption or subtotal annular disruption with extension of nucleus pulposus toward annular injury with expansive deformation. Represents a disk herniation (focal > broad-based) with extension of nucleus pulposus through zone of annular disruption with expansive deformation.
Disk herniation/extruded disk fragment–herniation/extrusion: Herniated fragment of nucleus pulposus without connection to disk of origin.
Disk herniations can be midline, off-midline in lateral recess, posterolateral within inter-vertebral foramen, lateral, or anterior. Can extend superiorly, inferiorly, or both directions; with or without associated epidural hematoma, with or without compression or displacement of thecal sac and/or nerve roots in lateral recess and/or foramen. Disk herniations can occur into the end plates of vertebral bodies, Schmorl nodes. |



























 10 Computed Tomography of Spinal Abnormalities
10 Computed Tomography of Spinal Abnormalities
 10 Computed Tomography of Spinal Abnormalities(Table 10.1 – Table 10.2)
10 Computed Tomography of Spinal Abnormalities(Table 10.1 – Table 10.2)
 10 Computed Tomography of Spinal Abnormalities(Table 10.3 – Table 10.4)
10 Computed Tomography of Spinal Abnormalities(Table 10.3 – Table 10.4)
 1 Brain and Extra-axial Lesions(Table 1.1 – Table 1.2)
1 Brain and Extra-axial Lesions(Table 1.1 – Table 1.2)
 15 Trauma and Fractures: Shoulder Girdle and Upper Extremity
15 Trauma and Fractures: Shoulder Girdle and Upper Extremity
 24 Gastrointestinal Tract
24 Gastrointestinal Tract



