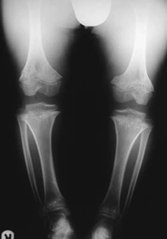
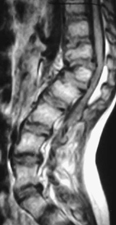
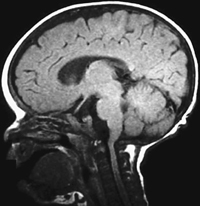
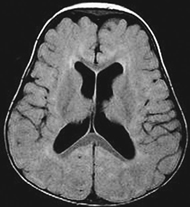
CASE 112 A healthy, active child presents with height well below fifth percentile for age. He demonstrates frontal bossing, generalized limb shortening with a relatively normal trunk, a mild “swayback” deformity, and spatulate hands. Figure 112A Figure 112B Figure 112C Figure 112D Figure 112E Figure 112F Figure 112G Lateral radiograph of lumbosacral spine (Fig. 112A) demonstrates anteroinferior beaking at L1 and L2, resulting in a mild gibbus. Distal lumbar lordosis is slightly exaggerated. The lumbar pedicles are quite short, resulting in spinal stenosis. Frontal radiograph of the pelvis (Fig. 112B) demonstrates short, squared iliac wings (“elephant ear” appearance), with horizontal acetabular roofs. The femoral necks are quite short, but the femoral heads are well developed. Note progressive narrowing of the distal lumbar interpediculate space. The hands (Fig. 112C) show mild generalized shortening of metacarpals and phalanges. Note the divergence of the fingers from one another (“trident hand”). Frontal view of the knees (Fig. 112D) demonstrates relative broadened distal femoral and proximal tibial metaphyses, with narrowing of the femoral intercondylar notch. The femora and tibiae are short and broad, and the fibulae are relatively elongated. Sagittal T2-weighted MRI of the lumbar spine (Fig. 112E) clearly demonstrates anterior upper lumbar beaking, with resultant gibbus deformity. Note compression of the conus medullaris at the T12-L1 disk interspace. Severe distal central lumbar canal stenosis is present; the lumbar cistern is not visible. Sagittal T1-weighted MRI of the brain just to the right of midline (Fig. 112F) demonstrates severe narrowing of the foramen magnum, with compression of the cervical cord at this level. Note mild frontal bossing. Axial short tau inversion recovery (STIR) weighted image demonstrates minimal prominence of the lateral ventricles (Fig. 112G). Achondroplasia Achondroplasia is the most common nonlethal skeletal dysplasia, seen in 1 in 26,000 live births. This condition has been long recognized and is represented in paintings from the Renaissance. Achondroplasia is an autosomal dominant condition caused by one of four distinct point mutations in the transmembrane domain region of fibroblast growth factor receptor 3 (FGFR3). This region is quite close to the defects seen in thanatophoric dysplasia type 1 and hypochondroplasia, both of which share many phenotypic and radiographic similarities with achondroplasia. Although most cases are the result of new mutations, vertical transmission is occasionally seen. Homozygous achondroplasia may be seen in children of two affected adults, demonstrating phenotypic severity between that of achondroplasia and thanatophoric dysplasia.
Clinical Presentation



Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Clinical Findings
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


