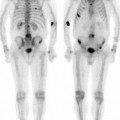
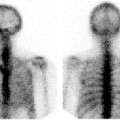
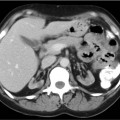
CASE 113 A 53-year-old woman with diabetes mellitus and end-stage renal disease presents with rising serum creatinine 2 months after receiving a cadaveric renal transplant. (A living related donor transplant had failed 8 years previously.) The postoperative course was complicated by febrile neutropenia. Multiple biopsies of the transplant kidney showed moderate-severe acute tubular necrosis but no evidence of rejection. Multiple CT examinations of the pelvis showed a stable 8.1 × 3.4-cm accumulation of fluid adjacent to the transplant kidney. Fig. 113.1 Fig. 113.2 Fig. 113.3 • 99mTc-MAG-3 (5-10mCi) is the radiopharmaceutical of choice because of its higher extraction fraction, although 99mTc-DTPA (10-20mCi) is an acceptable substitute. • Dynamic imaging of the pelvis for 20 or 30 minutes is followed by 10-minute static views, repeated as necessary for up to 2 hours. • For transplants located in the pelvis, imaging should be performed in the anterior view to avoid attenuation from the sacrum and pelvic bones. • When possible, correlation should be made with anatomic imaging (CT, MRI, or ultrasound) to evaluate any grossly evident fluid collections. Dynamic images (Fig. 113.1) show the transplant kidney in the left hemipelvis. Homogeneous perfusion is seen in the first frame, immediately after arrival of the injection bolus in the internal and external iliac arteries. There is slightly delayed tracer uptake in the renal cortex; however, no activity is seen in the renal pelvis, ureter, or bladder. The time-activity curves (Fig. 113.2
Clinical Presentation


Technique
Image Interpretation
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


