
Diagnosis: Epiploic appendagitis
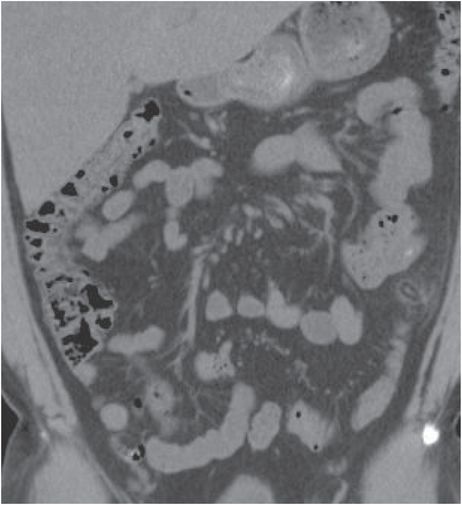
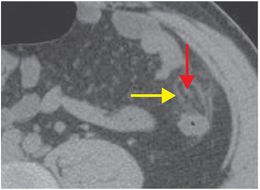
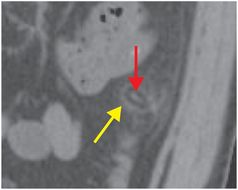
Axial (left image), sagittal (middle image), and coronal (right image) enhanced CT images of the abdomen and pelvis demonstrate a fat-density oval structure (yellow arrows) arising from the left colon. A central hyperdense focus (red arrows) represents a thrombosed vein. There is a small amount of peripheral mesenteric stranding.

Discussion
Overview of epiploic appendagitis
Epiploic appendages are small, fat-containing peritoneal outpouchings that arise from the serosal surface of the colon. Each epiploic appendage is connected to the colon by a vascular stalk, containing paired arterioles and a single vein.
Acute epiploic appendagitis is inflammation of an epiploic appendage, most commonly due to torsion that leads to central venous thrombosis and consequent ischemia.
Acute epiploic appendagitis is typically a self-limited condition and treatment is anti-inflammatory medications.
Acute epiploic appendagitis is more commonly adjacent to the left colon than to the cecum and right colon. There, the appendages are more numerous and longer, and thus, more prone to torsion. Less frequently, epiploic appendagitis may occur adjacent to the right colon and cecum.
Imaging of epiploic appendagitis
The CT appearance of acute epiploic appendagitis is characteristic and usually diagnostic. A typical appearance is a fat-density pericolic oval structure with surrounding inflammatory fat stranding. A central hyperattenuating focus representing the thrombosed vein is often present (the “central dot” sign), although epiploic appendagitis may still be diagnosed in the absence of this feature. The adjacent colon is usually normal, but mild reactive wall thickening may be seen.
Imaging and clinical differential diagnosis of epiploic appendagitis
Several conditions may mimic acute epiploic appendagitis, both clinically and on imaging, including omental infarction, mesenteric panniculitis, diverticulitis, and fat-containing tumor. When epiploic appendagitis involves the cecum, the condition may be mistaken for acute appendicitis. The distinction between epiploic appendagitis and other mimickers is crucial because epiploic appendagitis is a self-limited condition, whereas other conditions may require more definitive therapy. An adjacent inflammatory process may cause secondary inflammation of one or more epiploic appendages.
Clinical synopsis
The patient was diagnosed with acute epiploic appendagitis and was discharged home with pain medication only. She had improvement of her symptoms within a few days.
Self-assessment
|
|
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 32 32-year-old male complaining of chest pain after upper endoscopy
32 32-year-old male complaining of chest pain after upper endoscopy
 28 30-year-old male presented with a palpable left testicular mass
28 30-year-old male presented with a palpable left testicular mass
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


