15 Sonography of the Female Genital Tract
The female genital tract consists of the vagina, cervix, uterus, and ovaries. Pathology of the female genital tract in children is uncommon or often not yet apparent, and therefore an ultrasound (US) examination of this area is rarely requested. If requests are made in our university hospital, the examination in neonates is mostly for large ovarian cysts or ambiguous genitals, in young girls mostly for tumors, and in teenagers for tumors and amenorrhea.
US views of these structures are optimal when obtained through a filled or half-full bladder, which provides an acoustic window and pushes the air-filled bowels aside. If necessary, this can be accomplished in neonates by retrograde filling through a catheter. In neonates and small children, a linear high-frequency probe (4–12 MHz) gives high-resolution images; in larger children and adolescents, a curved array probe is used (3–6 MHz).
In the case of congenital anomalies, magnetic resonance (MR) imaging provides a better delineation of the anatomy than does US. Some of these anomalies are shown only with MR images.
15.1 Normal Anatomy and Variants
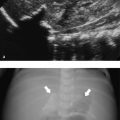
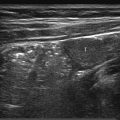
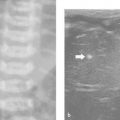
In the first days after birth, the uterus and ovaries of female neonates are remarkably prominent because of stimulation by maternal hormones. The cervix is equal in size to the fundus or slightly larger ( Fig. 15.1 ). The myometrium is thick, and the endometrial lining is visible ( Fig. 15.2 ). The ovarian follicles of the neonate may be large ( Fig. 15.3 ). After a few days, the size decreases and remains small for the next years. There will be a slow growth of these organs in relation to age and weight. During these years, the endometrium is usually not apparent and the follicles are small (up to 1 cm; Fig. 15.4 ). In the prepubertal years (usually from 9 years on), the uterus and ovaries increase in size more rapidly. The fundus grows larger than the cervix, which will cause a pear-shaped appearance ( Fig. 15.5 ). At puberty, the female genital tract will reach adult values, and the endometrium will be visible as an echogenic lining that varies with the phases of the menstrual cycle ( Fig. 15.6 ).






15.1.1 Normal Measurements
Normal values for the uterus and ovaries are shown in Table 15.1 . The volumes were calculated with the formula for an ellipsoid: length × width × height × 0.523.
Age | Number of healthy girls | Uterus, mL (SD) | Number of healthy girls | Ovary, mL (SD) |
0–1 month | 15 | 3.4 (1.2) | 6 | 0.5 (0.4) |
3 months | 7 | 0.9 (0.2) | 4 | 0.4 (0.1) |
1 year | 19 | 1.0 (0.2) | 6 | 0.5 (0.2) |
3 years | 26 | 1.0 (0.3) | 17 | 0.7 (0.4) |
5 years | 26 | 1.0 (0.3) | 13 | 0.7 (0.5) |
7 years | 28 | 0.9 (0.3) | 15 | 0.8 (0.6) |
9 years | 18 | 1.3 (0.4) | 12 | 0.6 (0.4) |
11 years | 16 | 1.9 (0.9) | 10 | 1.3 (1.0) |
13 years | 8 | 11.0 (10.5) | 8 | 3.7 (2.1) |
15 years | 15 | 21.2 (13.5) | 9 | 6.7 (4.8) |
Source: Van Rijn RR, Robben S. Normal values. In: Van Rijn RR, Blickman JG, eds. Differential Diagnosis in Pediatric Imaging. New York, NY: Thieme Medical Publishers; 2011:625–660. | ||||
15.2 Pathology
15.2.1 Congenital Anomalies
Congenital anomalies of the female genital tract are the result of abnormalities in the development of the paramesonephric (Müllerian) ducts, and to a much lesser degree the mesonephric (Wolffian) ducts, urogenital sinus, and/or cloaca. The upper parts of the paramesonephric ducts form the fallopian tubes. The lower parts fuse in the midline in a process called lateral fusion. They form the uterus and upper part of the vagina (Müllerian tubercle). The lower part of the vagina develops from the urogenital sinus. The lower part is separated from the upper part by the hymen, which thins and perforates in the perinatal period. The close relation of the paramesonephros with the mesonephros and metanephros makes a combination of genital and urinary tract anomalies likely. Therefore, during a US examination of the female genital tract in search of congenital anomalies, one should always visualize the kidneys and bladder as well. The reverse is also true; when a congenital renal anomaly, such as a horseshoe kidney, multicystic kidney, or duplex system, is detected, the uterus should be visualized as well because in approximately 10% of cases there will also be an abnormal formation of the genitals.
Müllerian Duct Anomalies
In considering the embryologic development of the female genital tract ( Fig. 15.7 ), congenital malformations in this area can be classified as follows:
Müllerian agenesis, in which there is a defect in the caudal portion of the Müllerian ducts;
Disorders of lateral fusion, in which the fusion of the two Müllerian ducts is incomplete; and
Disorders of vertical fusion, caused by malfusion between the Müllerian tubercle and urogenital sinus.

Fig. 15.7 Drawing of the embryologic development of the female genital system. The paramesonephric ducts (Müllerian ducts; arrow) fuse caudad to cephalad to form the proximal vagina and uterus. The unfused cephalic parts become the fallopian tubes. The caudal end comes in contact with the urogenital sinus (yellow; arrowhead). The vagina is formed partly by the urogenital sinus and partly by the paramesonephric ducts.
First category: In Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome, the vagina (or proximal two-thirds) is absent, in combination with absence or abnormalities of the uterus and frequently abnormalities of the urinary tract. In addition, the ovaries may be absent, malformed, or in a high location (maldescensus). The presentation is usually in pubertal girls with primary amenorrhea. MR imaging is needed to clearly visualize the rudimentary uterus and ovaries ( Fig. 15.8 , Fig. 15.9 , Fig. 15.10 ). There is an association with renal anomalies, and skeletal abnormalities may also occur.



Second category: When correct lateral fusion of the Müllerian ducts fails to occur, there will be a septate, bicornuate, didelphys, or unicornuate uterus ( Fig. 15.11 , Fig. 15.12 , Fig. 15.13 , Fig. 15.14 , Fig. 15.15 , Fig. 15.16 ). A minor fusion defect is a vertical septum in the vagina ( Fig. 15.17 ). Girls with these defects will often be asymptomatic until reproductive age ( Fig. 15.18 ). MR imaging is a better imaging modality than US to delineate the exact anatomy of these disorders.








Third category: Disorders of vertical fusion are imperforate hymen, transverse vaginal septum, and atresia of the cervix or vagina. Vertical defects may be obstructive, and therefore symptoms occur at an earlier age. Symptoms of hydrocolpos may develop after birth because of the accumulation of genital secretions. However, symptoms usually occur at puberty with cyclic abdominal pain without menstruation. Vertical fusion defects are associated with lateral fusion defects. Rarely, there is a triad of uterus didelphys, obstructed hemivagina, and ipsilateral renal agenesis, the Herlyn-Werner-Wunderlich syndrome ( Fig. 15.19 and Fig. 15.20 ).


Tips from the Pro
When a congenital anomaly of the kidneys is seen, visualize the female genital system as well to detect additional congenital anomalies.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


