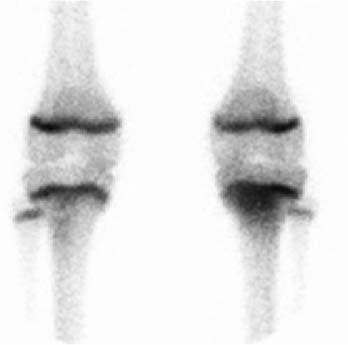
CASE 164 A 4-year-old boy presents with swelling and pain in his left leg for 2 days and fever and a limp for 1 day. There is no history of trauma. Radiographic evaluation of the left leg is within normal limits. Laboratory workup demonstrates a white blood cell count of 13,200/mm3 and a sedimentation rate of 48 mm/h. Blood cultures are obtained. Fig. 164.1 • 99mTc-MDP at 0.2 mCi/kg of body weight is given intravenously. The minimum dose is 1 mCi; the maximum dose is 20 mCi. • Use a high- or ultra-high-resolution, low-energy, parallel-hole collimator. Supplemental pinhole magnification images are obtained for improved detail. SPECT is performed for better three-dimensional localization. • The imaging time for an initial radionuclide angiogram is 3-second frames for 1 minute. A static blood pool image should be obtained within 5 to 10 minutes of tracer injection. A planar static view of the region-of-interest should be obtained 4 hours after injection. There should be whole-body or spot views of the entire skeleton. Fig. 164.2 An anterior radionuclide angiogram shows increased blood flow to the proximal left tibia (Fig. 164.1A). The distribution of increased tracer concentration depicted in the tissue phase imaging corresponds to the area with increased flow demonstrated on the radionuclide angiogram (Fig. 164.1B). Anterior views of the tibiae (Fig. 164.2) in the skeletal phase reveal abnormal uptake in the proximal left tibial metaphysis. • Osteomyelitis • Soft tissue infection/inflammation • Acute trauma • Malignancy • Sarcoidosis Following skeletal scintigraphy, bone biopsy was performed. Cultures grew Staphylococcus aureus (S. aureus). Intravenous antibiotic treatment was initiated based on a presumptive diagnosis of acute osteomyelitis. The patient’s condition improved on antibiotic treatment, and he was discharged in good condition after 1 week of hospitalization. He completed the course of antibiotic treatment as an out-patient. Acute osteomyelitis is a common pediatric problem. It usually results from the hematogenous spread of infection related to transient and often asymptomatic bacteremia. S. aureus is the most frequent infective organism.
Clinical Presentation
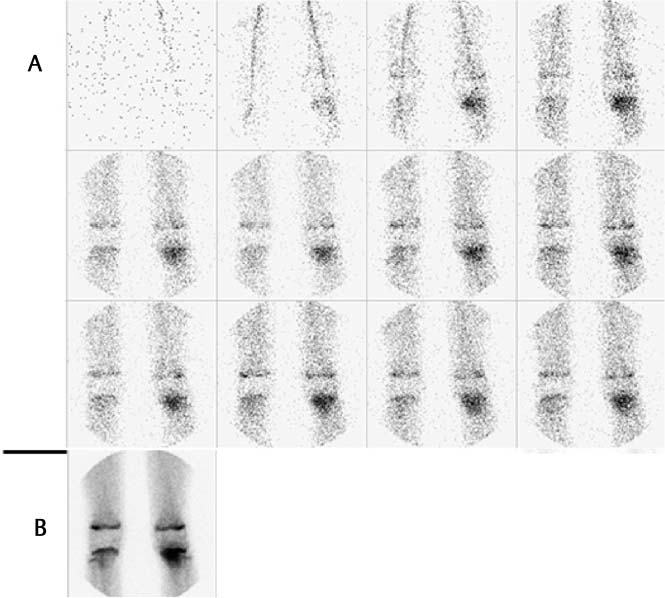
Technique
Image Interpretation
Differential Diagnosis
Diagnosis and clinical Follow-Up
Discussion
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


