
Diagnosis: Foramen of Winslow hernia containing incarcerated cecum
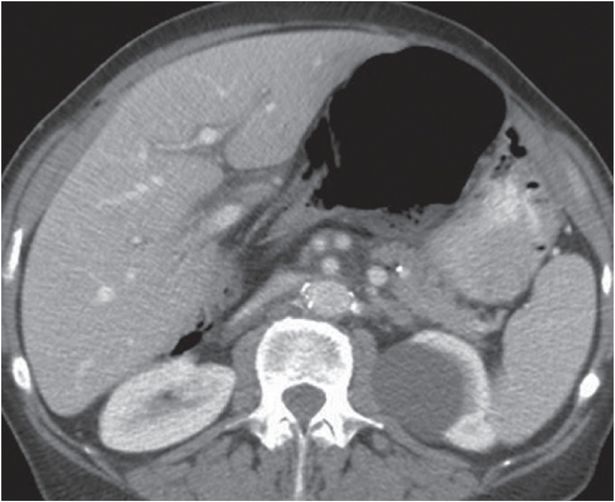
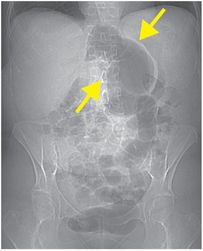
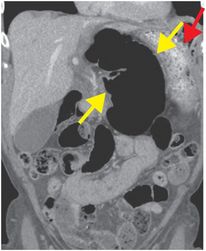
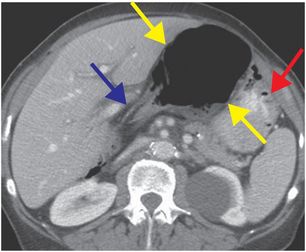
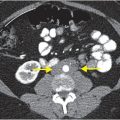
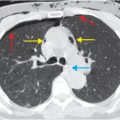
CT topogram (left image) and coronal IV and oral contrast-enhanced CT (middle image) show dilated, gas-filled cecum (yellow arrows) in the left upper abdomen displacing the stomach (red arrows) to the left. Axial contrast-enhanced CT (right image) shows the dilated gas-filled cecum in the lesser sac displacing the stomach posterolaterally. Stretched mesenteric vessels (blue arrow) pass posterior to the portal vein and anterior to the inferior vena cava (IVC) through the foramen of Winslow.
Discussion
The foramen of Winslow is a normal communication between the greater and lesser sacs. The borders include the IVC posteriorly, the caudate lobe superiorly, and the duodenum inferiorly.
The foramen of Winslow hernia is a congenital internal hernia that represents 8% of all internal hernias. Most foramen of Winslow hernias involve small intestine (60–70%), while the rest involve cecum and ascending colon. Rarely these hernias contain gallbladder, transverse colon, or omentum. Risk factors for herniation include an enlarged foramen, long small bowel mesentery, hypermobile right colon, and elongated right hepatic lobe.
Clinically, patients may present with symptoms of proximal bowel obstruction due to mass effect on the stomach. Symptoms are sometimes relieved by bending forward.
Characteristic CT findings include interposition of mesenteric fat and vessels between the IVC and liver hilum, air-distended bowel in the lesser sac with beaking directed towards the foramen of Winslow, displacement of the right colon from the right hemiabdomen, and anterolateral displacement of the stomach.
Clinical synopsis
Emergent diagnostic laparoscopy revealed a foramen of Winslow hernia with incarcerated cecum in the lesser sac. As this could not be reduced laparoscopically, the patient underwent open hernia reduction with resection of the ischemic-appearing right hemicolon. Pathologic analysis confirmed mucosal necrosis and ischemic changes of the cecum.
Related posts:
 8 67-year-old man with a history of altered mental status, left flank pain, and hypotension, on anticoagulant medications
8 67-year-old man with a history of altered mental status, left flank pain, and hypotension, on anticoagulant medications
 32 32-year-old male complaining of chest pain after upper endoscopy
32 32-year-old male complaining of chest pain after upper endoscopy
 28 30-year-old male presented with a palpable left testicular mass
28 30-year-old male presented with a palpable left testicular mass
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


