Gastrointestinal malignancies encompass a variety of primary tumor sites, each with different staging criteria and treatment approaches. In this review we discuss technical aspects of 18F-FDG-PET/CT scanning to optimize information from both the PET and computed tomography components. Specific applications for 18F-FDG-PET/CT are summarized for initial staging and follow-up of the major disease sites, including esophagus, stomach, hepatobiliary system, pancreas, colon, rectum, and anus.
Key points
- •
The usefulness of 18F-FDG-PET/CT scanning varies depending on the type of gastrointestinal tumor.
- •
PET combined with contrast-enhanced computed tomography scanning is particularly valuable for evaluating gastrointestinal tumors.
- •
Although not the primary imaging modality for most gastrointestinal malignancies, 18F-FDG-PET/CT scanning can guide therapeutic decisions when used strategically.
Introduction
Gastrointestinal (GI) malignancies encompass a wide range of disease sites, each with its own unique challenges. In organizing this review, we have chosen to divide the GI system into the following disease site categories: esophagogastric, colon, hepatobiliary, pancreas, and rectal–anal. We summarize 2-deoxy-2-[18F] fluoro-D-glucose positron emission tomography/computed tomography scanning (FDG-PET/CT) applications for initial staging and follow-up of these different GI malignancies, with particular attention to the role that FDG-PET/CT scanning plays in the management of these patients. Neuroendocrine tumors and small bowel tumors are not primarily evaluated by FDG-PET/CT, and are discussed in greater detail elsewhere in this issue.
General considerations
The usual patient preparation (fasting, glucose control, limiting exercise) is important for patients undergoing FDG-PET/CT imaging for GI malignancies. Oral contrast is frequently helpful for anatomic definition and lesion localization within the GI tract. Flavored, noncaloric barium preparations can be used, which the patients can sip during the FDG uptake phase. Neutral oral contrast such as water can also be used before imaging pancreatic lesions. Metformin can result in high FDG activity throughout the bowel, making it difficult to identify underlying lesions. Having patients discontinue metformin for 24 to 48 hours before FDG-PET/CT scanning can decrease this artifact, but is usually not practical owing to the risk of hyperglycemia.
Intravenous contrast can also be beneficial for anatomic localization and diagnosis, especially for FDG-PET/CT evaluation of the liver and pancreas. Newer generation multidetector PET/CT scanners are capable of providing thin-slice multiphase CT scans in the arterial and portal venous phases of enhancement. If contrast-enhanced CT is not performed concurrently as part of the FDG-PET/CT study, it is important to correlate the FDG-PET findings with a separate contrast-enhanced CT or MR scan.
Esophageal cancer
Initial Staging
Esophageal cancer comprises squamous cell carcinoma (in the proximal two-thirds esophagus) and adenocarcinoma (distal third and esophagogastric junction [EGJ]). Its incidence has been increasing, owing to the greater frequency of adenocarcinoma arising in the squamous metaplasia of Barrett’s esophagus, with an estimated 19,260 new cases and 15,530 deaths in the United States in 2021. Except for cervical esophageal cancer, for which definitive chemoradiation is used, surgical resection with lymphadenectomy is the best curative therapy in patients without distant metastases. However, morbidity is high, and imaging is critical to help select only those patients who will benefit from esophagectomy. With conventional imaging, metastatic disease is found during surgery in as many as 60% of patients, and more accurate staging with advanced imaging is needed.
Although pathologic staging best correlates with survival, FDG-PET/CT scans, endoscopic ultrasound (EUS) examination, and CT scans have improved the accuracy of clinical staging. FDG-PET/CT scanning from the skull base to the mid-thighs is currently recommended for initial staging of esophageal and EGJ cancers unless there is known metastatic disease. FDG-PET/CT scanning is more sensitive than CT alone for detecting metastasis and therefore allows better patient selection for surgical resection. In a prospective multicenter trial, FDG-PET/CT scanning found metastases in 41% and changed management in 38% of cases. Limitations of FDG-PET/CT scanning include a decreased sensitivity for detection of liver metastases if the CT component is without intravenous contrast and potential false-positive findings.
FDG-PET/CT scanning has limited ability to differentiate between clinical (c)T1, T2, and T3 tumors , and plays no role in T staging, except for possibly determining mediastinal invasion. FDG-PET scanning has less usefulness in early stage (cT1) tumors because of a low prevalence of metastatic disease and risk of false-positive findings. , FDG-PET/CT scanning sensitivity compared with endoscopy in a screening setting was found to be 4% and it is not useful for this purpose. Although focal FDG avidity in the esophagus is most often malignant, uptake in esophageal papilloma may be a false positive finding. FDG-PET/CT scanning is helpful in delineating the target volume before radiation therapy; a small study determined that respiratory-gated CT scanning underestimated the size of the target volume by 20% when compared with FDG-PET/CT scanning. The metabolic tumor volume (MTV) on a baseline FDG-PET/CT scan before neoadjuvant chemotherapy correlated with pathologic response in 61 patients with squamous cell and adenocarcinoma of the esophagus.
For nodal staging, EUS examination is superior for assessment, having an 85% sensitivity, with additional fine needle aspiration improving cN staging sensitivity and accuracy. CT scan sensitivity is 30% to 60% using a node long axis of greater than 1 cm. , In a large meta-analysis of studies originating in Asia, the pooled sensitivity and specificity for the detection of regional lymph node metastasis was 66% and 96%, respectively. In a retrospective review of 148 patients with esophageal cancer, FDG-PET scanning did not alter nodal staging in any patient who had undergone complete EUS–fine needle aspiration.
In esophageal squamous cell carcinoma, FDG-PET/CT scanning performs similarly to EUS examination in discriminating N0 from N1 disease, while being slightly more sensitive but otherwise similar to EUS for distinguishing T1a or less disease from other tumors. The most commonly involved lymph nodes in upper esophageal cancer are supraclavicular, retrotracheal, and paratracheal, whereas the most common in lower esophageal cancer are paraesophageal and gastrohepatic nodes. FDG-PET/CT scanning is useful before endoscopy, helping to delineate nodal distribution before fine needle aspiration.
In a novel study of 20 patients with mostly squamous cell histology, FDG-PET imaging was performed on the same day before surgical resection with lymph node dissection. Radioactivity in the harvested lymph nodes was measured using a well counter and correlated with pathology. Lymph node analysis from PET images yielded sensitivity, specificity, positive predictive value, and negative predictive value of 29%, 97%, 44%, and 94%, respectively. Ex vivo counts were more accurate, yielding 95%, 79%, 14%, and 99.8%, for these respective parameters. The authors suggested that FDG uptake in nodes may be helpful in navigation surgery for esophageal cancer.
Mining PET data to find radiomic signatures predictive of outcomes is a burgeoning area of research in esophageal cancer. Yip and colleagues found that PET-based textural features (entropy and run–length matrix) correlated with outcome after neoadjuvant chemotherapy, better than the standardized uptake value (SUV). Convolutional neural network analysis of FDG-PET/CT scans was used to predict lymphovascular invasion and perineural invasion in 798 patients with esophageal squamous carcinoma. In 65 patients with esophageal cancer treated with chemoradiation and followed for 3 years, pretreatment FDG-PET scans and medical records were analyzed using a random forest machine learning approach; the MTV was found to be the strongest predictor of response and survival.
With the rapid technological changes in PET/CT scanners (time-of-flight resolution and advanced reconstruction techniques), previous assumptions regarding PET quantitation vis-à-vis the maximum (SUV max ), and data in older literature, will need to be reassessed. In particular, SUV has limitations, such as body composition, glucose level, uptake time, and reconstruction parameters, and sometimes can be misleading; there has been greater interest in qualitative scoring paradigms across a range of tumor types, and esophageal cancer is no exception.
Huang and colleagues applied a qualitative 4-point scale to FDG-PET analysis: 1, no focal uptake; 2, focal uptake greater than surrounding tissue or blood pool but equal or less than the liver; 3, diffuse uptake greater than blood pool up to marginally greater than liver; and 4, focal uptake much greater than liver. Scores of 1 to 3 were viewed as negative and a score of 4 was positive. Taking into account multiple parameters derived from the postchemoradiation FDG-PET scan, including above and below the median values of the SUV max , the percent change in SUV max , and MTV, only the American Joint Commission on Cancer stage and qualitative 4-point scale to FDG-PET analysis score significantly correlated with overall survival on multivariable Cox regression analysis. In a retrospective study of 128 patients with esophageal squamous cell cancer by Wang and colleagues it was found that a tumor-to-liver SUV ratio was superior to SUV max and tumor-to-blood pool ratio by receiver operating characteristic analysis in predicting tumor response and survival after chemoradiation.
Interim assessment
Several keys studies have revealed a potential role for FDG-PET/CT scans in identifying responders early (ie, 14 days) during neoadjuvant chemotherapy, thereby sparing nonresponding patients a toxic therapy without clinical benefit and allowing them to be resected sooner. , MUNICON II, a prospective trial of 56 patients with EGJ adenocarcinoma showed that event-free and overall survival was significantly shorter in metabolic nonresponders compared with metabolic responders, with a metabolic response defined as a 35% or greater decrease in the SUV on FDG-PET scanning 2 weeks into neoadjuvant chemotherapy. Metabolic responders continued neoadjuvant chemotherapy for up to 12 weeks, and nonresponders received salvage radiochemotherapy before resection. In a study of 134 patients with squamous cell cancer by Li and colleagues, where FDG-PET was performed before and during neoadjuvant chemoradiation, SUV max was found to be an independent prognostic factor for OS by Cox regression analysis, complementary to length of tumor and TNM stage. Other studies have shown similar results.
In the ongoing phase II CALGB 8083 trial, patients with resectable esophageal and EGJ adenocarcinoma (n = 257) had their chemotherapy during neoadjuvant chemoradiation changed based on a greater or less than 35% decrease in SUV on FDG-PET scanning. Preliminary data indicate that this led to improved pathologic complete response rates in metabolic responders compared with nonresponders.
Preoperative Assessment
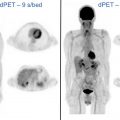
Preoperative chemoradiation is a category 1 recommendation for locally advanced squamous cell carcinoma or adenocarcinoma of the thoracic esophagus or EGJ by the National Comprehensive Cancer Network (NCCN). FDG-PET/CT scanning from the skull base to mid-thigh is recommended in the NCCN guidelines for assessment after neoadjuvant or definitive chemoradiation in both squamous cell carcinoma and adenocarcinoma, in part to exclude the development of metastatic disease. Many studies have shown that decreased uptake of FDG is predictive of survival in patients with locally advanced esophageal or EGJ cancer who undergo neoadjuvant treatment. , However, the exact cutoff values for absolute decrease and percent change in SUV between pretreatment and post-treatment scans varied widely between studies. In a report by Cerfolio and colleagues, a decrease in SUV of more than 64% correlated with a complete pathologic response. Smith and colleagues found that a decrease in SUV of more than 50% conferred a 12-month disease-free survival advantage over those patients who had a decrease in SUV of less than 50% (93% vs 43%). Kukar and colleagues, in a retrospective study of 77 patients with adenocarcinoma who underwent PET scanning before and after neoadjuvant chemoradiation, found that pretherapy SUV, and change in SUV were significantly higher in patients who achieved complete pathologic response. A change in SUV of less than 45% was associated with residual disease. Fig. 1 shows an EGJ adenocarcinoma with celiac nodal metastases that responded to neoadjuvant chemoradiation and correlated with a complete pathologic response. In many of these studies, the PET response did not correlate well with the pathologic response, with microscopic disease still present in metabolic responders. Accordingly, surgery is still recommended even if a strong postneoadjuvant therapy metabolic response is observed on PET.

Elevated FDG uptake in lymph nodes after neoadjuvant chemotherapy is highly specific (99%) but not sensitive (12%) in identifying nodal metastases. As discussed elsewhere in this article, textural features of PET data are an emerging area of research and may be predictive of outcomes in esophageal cancer. In a retrospective study by Simoni and colleagues, 54 patients with adenocarcinoma and squamous cell carcinoma underwent FDG-PET/CT scanning before and after induction therapy, and then again after neoadjuvant chemoradiation and surgery. In addition to MTV and TLG, 3 radiomic features extracted from the pre-induction PET scan were correlated significantly with a pathologic response.
Although other studies have indicated limited usefulness of FDG-PET for the assessment of response to neoadjuvant therapy in esophageal cancer, many of these were likely confounded by false-positive PET findings, with FDG-PET scanning performed during or soon after preoperative therapy. , Radiation and chemoradiation may cause local inflammation in the esophagus, limiting the usefulness of FDG-PET scans in early response assessment of esophageal cancer. Accordingly, the NCCN guidelines recommend that FDG-PET/CT scanning should be performed at least 5 to 8 weeks after the completion of neoadjuvant chemoradiation.
Post-treatment Follow-up
For patients with esophageal cancer who recur locoregionally and are treated with esophagectomy and/or chemoradiation, a CT scan is recommended as follow-up, but not an FDG-PET/CT scan, unless distant disease is suspected. For surveillance, a CT scan is recommended. Although not recommended in the NCCN, FDG-PET/CT scanning may still be useful in follow-up: a meta-analysis by Goense and colleagues of 486 patients with esophageal cancer after treatment with curative intent found FDG-PET/CT to detect recurrence with a pooled sensitivity and specificity of 96% and 78%, respectively.
Gastric cancer
Initial Staging
Approximately 26,560 new cases of gastric cancer are estimated for 2021 in the United States, with 11,180 deaths. The 5-year survival rate is 70% for localized tumors, 32% once spread locoregionally, and 6% with distant metastases. Of gastric cancers, 95% are adenocarcinomas and classified as either proximal (about the cardia) or distal, and either diffuse or intestinal in histologic type. The diffuse type, typified by tumor cells scattered within a fibrous stroma, is mostly associated with low-risk areas and gene mutations. Intestinal type is found in high-risk areas and is associated with Helicobacter pylori infection, smoking, and dietary factors including heavy alcohol intake. Tumors having an epicenter located more than 2 cm into proximal stomach are staged as gastric carcinomas, whereas those involving the EGJ with the epicenter less than 2 cm into the proximal stomach are staged as esophageal cancers.
Tumors in the lower two-thirds stomach are treated with subtotal gastrectomy; otherwise, total gastrectomy is recommended. For small, early gastric cancer confined to the mucosa, endoscopic resection is appropriate. Once it has invaded the submucosa (T1b), radical gastrectomy and lymphadenectomy are required. Locally advanced gastric cancer without distant metastases may be treated with surgical resection and perioperative chemotherapy. Despite advances in imaging and treatment, the 5-year survival is 25% to 30%, with EGJ (cardia) and diffuse-type noncardia gastric cancer having the worst prognosis.
The current NCCN guidelines recommend CT scans of the chest, abdomen, and pelvis with oral and intravenous contrast as the primary modality for initial staging of gastric cancer, with FDG-PET/CT scans used for confirmation if there is no evidence of M1 disease. EUS examination is used for assessing early stage disease, particularly depth of tumor invasion and local nodal involvement, although its accuracy is limited (46% and 67%, for these respective parameters). CT scanning is 43% to 83% accurate for T staging. In a retrospective study of 229 patients with early stage gastric cancers by Yoon and associates, FDG uptake was detected in only 18% of patients and found to depend on location (distal stomach with higher uptake), size, and depth of invasion. Diffuse and mucinous tumor types often demonstrate low FDG uptake, contributing to lower accuracy of FDG-PET scans compared with CT scans. , In a retrospective review of 105 patients with gastric cancer who underwent preoperative staging, 14% of tumors were not metabolically active, and intestinal subtype correlated with s higher SUV max than nonintestinal, and FDG-PET scanning upstaged 19% of patients, with the majority a result of hitherto unknown distant metastases.
The SUV max of FDG in the primary tumor was found to be associated with the degree of differentiation, with the signet ring histology often being negative. This finding is likely secondary to a decreased expression of GLUT1 in the signet ring cell subtype. In a study of 341 patients with gastric cancer, FDG uptake was greatest in medullary and tubular subtypes, and lowest in signet ring, although when high uptake by SUV max was observed in signet ring cell carcinoma, a greater likelihood of regional and distant metastatic disease was found. The PET scan detection rates range from 40% to 90%, owing to this variable histology. , , Accordingly, FDG-PET scanning may not be appropriate as initial evaluation for T1 disease. FDG-PET scanning is less sensitive, but more specific compared with CT scans for local nodal involvement, and FDG-PET/CT scanning is more accurate in preoperative staging (68%) than PET scanning (47%) or CT scanning (53%) alone.
When FDG avidity is observed, it is prognostically significant. In a large meta-analysis of 1,080 patients by Wu and coworkers, high pretreatment SUV was prognostic, with hazard ratios of 1.7 for overall and recurrence-free survival. A high SUV max and high MTV correlated with a higher risk of recurrence in advanced gastric cancer before curative surgery. In a large study of 566 patients with gastric cancer by Song, a nomogram was developed and found that tumor SUV max and nodal SUV max on preoperative PET/CT scans were independent predictors for lymph node metastases, with a further improvement in prediction found when albumin and carbohydrate antigen 19-9 were also used. In a study of 168 patients, Kwon and colleagues found that FDG avidity of lymph nodes (defined as focal uptake on visual inspection and by MTV) was an independent predictor of recurrence-free survival, although avidity of the primary tumor was not—possibly reflecting confounding heterogeneous histology and background gastric wall uptake.
A pitfall of FDG-PET interpretation is inflammatory gastric activity, which can be focal as well as diffuse. Indeed, 1 study of 88 patients, performed in a Japanese PET/CT cancer screening program, found FDG uptake useful in predicting H pylori infection and subsequent atrophic gastritis (a risk factor for cancer). Uptake was higher in the gastric fundus than other areas of the stomach, but not significantly correlated with pathology. Interestingly, of the 4 early gastric cancers detected, none had increased FDG uptake. Less common false positives include IgG4-related disease and myofibroblastic sarcoma of the gastric cardia.
Subsequent Treatment Strategy
In patients who cannot undergo surgery and receive primary chemotherapy or radiation, post-treatment assessment is usually performed with CT scans, although FDG-PET/CT scanning is recommended in patients who have renal insufficiency or are allergic to iodinated contrast. FDG-PET/CT scanning may be used in follow-up for pathologic stage II to III disease or stage I to III disease after neoadjuvant or adjuvant therapy, although CT scanning every 6 to 12 months for the first 2 years, then every year for 5 years, is standard practice at many institutions. EUS examination performed better than PET/CT scanning in gastric cancer restaging (89% vs 69% accuracy) before resection in a group of patients, 80 of whom then had neoadjuvant chemotherapy and 100 who proceeded directly to surgery.
FDG-PET/CT scanning likely has value in the assessment of response after perioperative chemotherapy or preoperative chemoradiation (which is used in cT2 or higher, any N, M0 disease). In a study of 21 patients, the percent change in the SUV was the best-performing PET parameter after neoadjuvant therapy in distal esophageal and gastric adenocarcinomas; however, the pathologic response by histologic grading was still found to be a better predictor of survival than FDG uptake. In a retrospective study by Schneider and colleagues of 72 patients with gastric cancer or EGJ or gastric cardia (Siewert II or III) cancers, patients were enrolled who underwent FDG-PET before, and 14 days after the first of 3 cycles of neoadjuvant chemotherapy. Metabolic response was defined as a 35% or greater decrease in the SUV max . The presence of a metabolic response did not correlate with pathologic response (ie, one-half had a major and one-half had minor pathologic regression), whereas in metabolic nonresponders, 90% had minor and 10% had major regression.
These results suggest that FDG-PET scans may identify patients who should immediately go to surgery or receive multimodality therapy. In a prospective study of 20 patients with gastric cancer by Won and colleagues, the authors demonstrated that a response similar to metabolic responders could be recovered in metabolic nonresponders if chemotherapy were switched after the postcycle 1 PET scan showing no metabolic response. Upon tumor recurrence, high FDG uptake by SUV max on PET/CT scanning was found to correlate with worse 3-year postrecurrence survival in work by Kim and colleagues.
Hepatocellular carcinoma
Hepatocellular carcinoma (HCC) is the sixth most common cancer in the world, with 42,220 new cases and 30,200 deaths in the United States in 2018. , The diagnosis of HCC is made when certain CT scan or MR imaging features (Liver Reporting & Data System 5) are encountered in high-risk patients (eg, cirrhosis, chronic hepatitis B, or prior HCC). For equivocal findings (Liver Reporting & Data System 2–4), a biopsy or additional imaging may be used.
FDG-PET/CT scanning is not recommended for routine initial imaging owing to its limited sensitivity, which likely results from lower tumor GLUT1 expression and a high concentration of glucose-6-phosphatase in normal liver, leading to rapid clearance of FDG and decreased contrast between normal parenchyma and well-differentiated HCC. In a prospective study by Park and colleagues of 99 patients with HCC, sensitivity for detection of HCC was only 61%, although it increased with tumor size and multiplicity and poorly differentiated histology, and the overall survival rate was lower in FDG-positive patients. FDG positivity in HCC has been reported between 38% and 70% with an overall sensitivity of 60%.
FDG-PET scanning does have high specificity in HCC, and may be used to evaluate an equivocal imaging finding. An HCC detected by CT scanning/MR imaging with high FDG uptake by SUV likely is more biologically aggressive and less likely to respond to locoregional therapies. A meta-analysis of 1,721 patients showed that FDG-PET/CT scanning may be useful in predicting overall and disease-free survival rates, but is of low sensitivity for HCC detection.
FDG-PET has high sensitivity for detection of extrahepatic metastases, approaching 100%, and detects recurrences earlier than conventional imaging. , In a small study of 34 patients with HCC who underwent FDG-PET/CT scanning before Y-90 radioembolization, FDG avidity in HCC was associated with a shorter time to progression within treated lesions and within more distant lesions in the liver, as well as a shorter progression-free survival rate after Y-90 radioembolization.
An emerging role for FDG-PET/CT scanning in HCC is the workup for liver transplantation, which is the ideal therapy for HCC because it can remove both the HCC and the underlying tumor-generating cirrhosis. The selection of patients with HCC for liver transplant has traditionally been performed by the Milan criteria, which require (1) 1 lesion smaller than 5 cm or up to 3 lesions smaller than 3 cm, (2) no extrahepatic disease, and (3) no vascular invasion. However, the Milan criteria are restrictive and do not include other factors that reflect tumor biology.
Although HCC vascular invasion is a major determinant of post-liver transplant outcomes, its detection requires invasive tissue sampling, which carries a higher risk in these patients. Several studies have shown that tumor differentiation independently predicts recurrence and survival after transplantation. FDG uptake is a sensitive and specific indicator for poorly differentiated tumors and has been found to be predictive of vascular invasion in HCC. ,
A large Japanese multicenter study of 182 liver transplant recipients found that those patients who did not conform to the Milan criteria recurred at a much higher rate at 5 years relative to those who were within Milan criteria (38% vs 7%, respectively); however, there was a subgroup of patients outside of Milan criteria with a negative PET/CT scan and low alpha fetoprotein who did just as well as recipients who were within the Milan criteria. Many studies have shown FDG negativity in HCC before transplantation to be strongly predictive of high disease-free survival rates. Consequently, there has been recent development of expanded liver transplant criteria that incorporate FDG-PET metabolic information, for example, the National Cancer Center Korea criteria. FDG-PET/CT scanning is not routinely recommended for post-treatment assessment in HCC.
Biliary tract cancers
Gallbladder Cancer
Gallbladder cancer is a rare cancer, with approximately 9700 cases per year in the United States. The 5-year survival rate is 50% for stage 1 disease, and less than 10% for stage III and above. It grows rapidly, invading the liver and spreading to lymph nodes, hematogenously, and intraperitoneally, and is often detected at a late stage. Complete resection is possible for early disease (T1–2, N0), and distant metastasis and N2 disease are contraindications to surgery. Management includes cholecystectomy with partial hepatectomy, chemotherapy, radiation therapy, and endoscopic stenting.
FDG-PET/CT imaging of gallbladder cancer is not commonly performed, with ultrasound examination, CT scanning, and MR imaging being the mainstays for evaluation. A meta-analysis examining the diagnostic accuracy of FDG-PET/CT scanning for gallbladder cancer reported sensitivity of 87% (95% confidence interval, 82%–92%) and specificity of 78% (95% confidence interval, 68%–86%), with an area under the curve of 0.88. Recent retrospective studies indicate that FDG-PET scanning may be useful for detecting regional nodal or distant metastatic disease, which is occult on CT scanning in patients who would otherwise be resectable. Leung and colleagues studied 100 patients with 63 gallbladder cancers and found the sensitivity and specificity of FDG-PET scanning to be 56% and 94%, respectively. FDG-PET scanning found malignancy not seen on CT scanning in 3 patients, and confirmed benignity in 2 patients with suspicious CT findings. The impact was greater in patients without prior cholecystectomy and when evaluating findings suspicious for nodal disease on CT scanning. Gallbladder inflammation and infection are potential false positives. ,
Cholangiocarcinoma
Cholangiocarcinoma is the second most common primary hepatic cancer; most tumors arise at the liver hilum (Klatskin tumor), and the others arise in the distal common bile duct or intrahepatic ducts of the liver (intrahepatic cholangiocarcinoma). The 5-year survival rate for resectable disease ranges from 22% to 44%. Survival is related to size and number of tumors, lymph node metastasis, and invasion of the vasculature. Peritoneal spread is present in 10% to 20% of patients at presentation and precludes surgical resection.
Lee and associates retrospectively reviewed the diagnostic and prognostic role of FDG-PET/CT scans in 76 patients with intrahepatic cholangiocarcinoma. FDG-PET/CT scanning was more sensitive for detecting nodal metastasis than CT scanning or MR imaging (74.5% vs 61.8%) and identified distant metastases occult on other modalities in 6 patients. Higher measures of FDG uptake (SUV max , MTV, TLG) were correlated with significantly reduced survival. Other retrospective studies indicate that PET scans may be useful for detecting regional nodal or distant metastatic disease, which is occult on CT scans, in patients who would have otherwise resectable disease. , , FDG uptake on preoperative PET scan by MTV is associated with K-ras mutation.
Extrahepatic cholangiocarcinoma includes common bile duct cancer and Klatskin tumor, and carries a high mortality. Surgical resection and lymph node dissection can confer long-term survival; however, this is only possible with accurate staging. FDG-PET/CT scanning is not routinely recommended for evaluation; however, recent reviews have demonstrated diagnostic and prognostic usefulness. In a retrospective review of 234 patients with extrahepatic cholangiocarcinoma by Kim and coworkers, FDG-PET/CT scanning was compared with contrast-enhanced CT scanning and MR imaging. FDG-PET/CT scanning was performed to characterize indeterminate primary tumor lesions or findings equivocal for nodal and distant metastases on other imaging. The PET sensitivity for detection of primary tumor was inferior to CT scanning or MR imaging (78.6% vs 95.0%–97.0%), as it was for detection of nodal metastasis (44% vs 75%–78%). By multivariate analysis, the SUV max of the primary tumor and metastatic disease was associated with poorer overall survival (hazard ratios of 1.75 and 8.1, respectively). When focusing on the periductal infiltrating subtype of extrahepatic cholangiocarcinoma, an SUV max of greater than 5 in the primary tumor was associated with an increased risk of nodal and distant metastasis (odds ratios of 1.6 and 101, respectively) and a hazard ratio of 1.8 of poor overall survival.
Pancreatic cancer
Initial Staging
Pancreatic ductal adenocarcinoma (PDAC) is the second most common GI cancer after colorectal cancer in the United States, with approximately 60,430 new diagnoses and 48,220 deaths expected in 2021. It has remained one of the most lethal cancers in the world, with a dismal 5-year survival of 5%, primarily owing to advanced stage at presentation. The standard of care for resectable tumors is surgery followed by adjuvant chemotherapy; however, less than 20% are resectable at diagnosis. Selected patients at risk for positive margins will now undergo neoadjuvant therapy, which may downstage tumors so that they may be resected. In stage 1 disease, the tumor is confined to the pancreas; in stage 2, the tumor extends outside the pancreas but without vascular involvement; in stage 3 disease, there is vascular involvement; and in stage 4, there is distant metastatic disease.
Multidetector, contrast-enhanced pancreas protocol CT scanning is the preferred initial imaging modality for PDAC. Typically, arterial and parenchymal phase images are acquired with thin slices and multiplanar reconstruction to define vascular anatomy that is critical for surgical planning. However, FDG-PET/CT scanning should be considered in high-risk patients to detect metastatic disease outside the pancreas. High-risk indicators include borderline resectable disease, marked elevation of carbohydrate antigen 19-9, large primary tumors, large regional lymph nodes, and severe clinical symptoms.
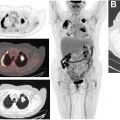
At diagnosis, FDG-PET scanning can distinguish between benign and malignant pancreatic lesions, especially when combined with EUS examination, although inflammatory disease is a source of false positives. A prospective study by Buchs and colleagues of 45 patients showed 96% sensitivity but 67% specificity for detection with contrast-enhanced PET/contrast-enhanced CT scanning , which decreased to 72% and 33% when PET/CT scanning was performed without intravenous contrast. Fig. 2 shows an example of a small ampullary adenocarcinoma on FDG-PET/CT scanning and the importance of contrast enhancement. In a prospective study of 108 PDAC patient PET scans, the accuracy rate was 80% for local invasion, 94% for distant metastasis, and 42% for lymph node spread.