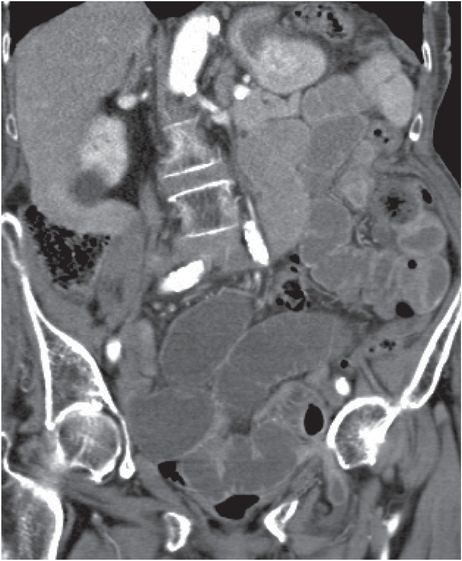
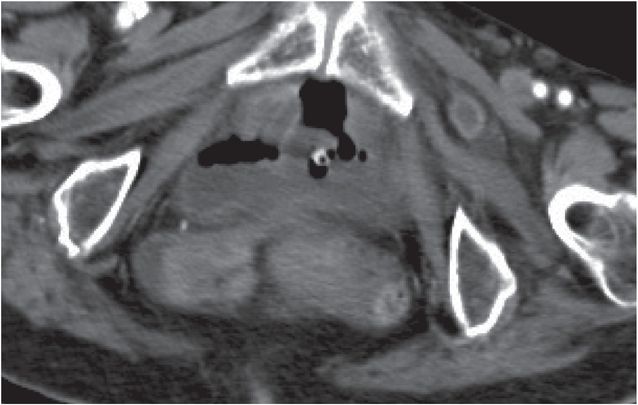
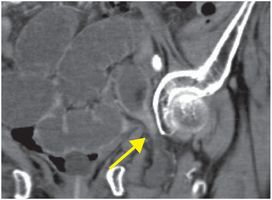
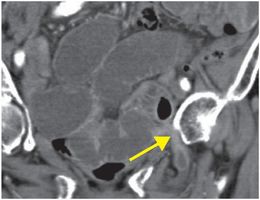
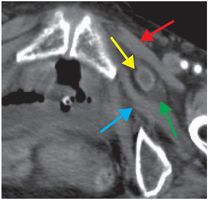
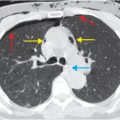
Diagnosis: Incarcerated left obturator hernia
Coronal and axial CT images with oral and IV contrast demonstrate multiple dilated loops of small bowel with tapering (yellow arrows; left and middle images) at the level of the obturator foramen. The incarcerated loop (yellow arrow; right image) is visible between the pectineus (red arrow) and obturator externus (blue arrow) muscles. Fluid (green arrow) in the hernia sac raises concern for strangulation.
Discussion
Overview of external hernia
External hernias are characterized by herniation of bowel outside of the normal confines of the peritoneal cavity. They are typically asymptomatic and often electively repaired. External hernia repair is the most commonly performed general surgical procedure in the United States.
Complications of external hernia include bowel obstruction, incarceration (irreducible sac), and strangulation (ischemia).
An obturator hernia is a relatively uncommon form of external hernia most commonly occuring in elderly females. Bowel obstruction is common. Recognition of obturator hernia is important as a strangulated obturator hernia has the highest mortality rate of all hernias. Obturator hernias occur in between the pectineus and obturator externus muscles, as demonstrated in the above case.
Imaging of external hernia
CT is the imaging modality of choice for evaluation of suspected external hernia.
External hernias that are difficult to palpate due to patient body habitus or anatomic location (as in obturator hernia) may be readily diagnosed by CT. CT can distinguish an abdominal wall hernia from other palpable masses including abdominal wall neoplasms, rectus sheath hematomas, varices, and inguinal lymphadenopathy.
Complications of external hernia, including small bowel obstruction and ischemia, are well evaluated by CT. CT findings of early bowel compromise include adjacent fat stranding or fluid in the hernia sac. CT findings of ischemia include pneumatosis intestinalis, portal venous gas, or pneumoperitoneum; however, it is important to note that pneumatosis and portal venous gas may also be “benign” (i.e., non-ischemic in etiology).
Clinical synopsis
The patient underwent laparoscopic reduction of the incarcerated hernia. The defect was repaired with mesh. There was no evidence of bowel ischemia at the time of surgery.
Self-assessment
|
|
|
|
|
|
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 32 32-year-old male complaining of chest pain after upper endoscopy
32 32-year-old male complaining of chest pain after upper endoscopy
 28 30-year-old male presented with a palpable left testicular mass
28 30-year-old male presented with a palpable left testicular mass
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


