23 Oral Cavity
23.1 Oral Cavity, Salivary Glands, and Pharynx
The oral cavity is the gateway for food into the body and is involved with breathing and verbal communication, and consequently it may serve as the point of entry into the body for infectious agents. Against this, physical barriers (the tongue, glottis, etc.) and immunologic barriers (Waldeyer’s ring of lymphatic tissue) serve to protect the airway and the body from unwanted intruders. The salivary glands provide lubrication, pH buffering, and antibacterial substances to help maintain normal functions and prevent infection. Lesions of the oral cavity and pharynx in children are of infectious etiology much more often than in adults, in whom neoplastic lesions of these structures are the primary concern. However, just as adults can get infections, neoplasms can develop in children.
23.2 Anatomy
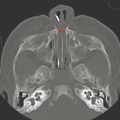
The oral cavity is bounded anteriorly by the lips, inferiorly by the tongue and floor of the mouth, superiorly by the hard and soft palates and dental arches, and laterally by the buccal mucosa, and communicates posteriorly with the oropharynx (Fig. 23.1). The posterior portion of the oral cavity is bounded laterally by the palatine tonsils and palatal and pharyngeal folds (Fig. 23.2). Posteriorly, the oral cavity communicates with the oropharynx, which is inferior to the nasopharynx and superior to the hypopharynx.


The parotid glands are superficial to the masticator space and anteromedial to the sternocleidomastoid muscle. The submandibular glands are located in the submandibular triangle beneath the inferior border of the mandible, and wrap around the posterior edge of the mylohyoid muscle to enter the floor of the mouth. The sublingual glands are adjacent to the base of the tongue in the floor of the mouth. Additionally, the oral cavity contains thousands of minor salivary gland ducts.
A brief mention of the location of the salivary gland ducts is important because they are the sites of certain pathologies. The parotid duct (Stensen’s duct) pierces the buccinator muscle and empties into the oral cavity through the buccal mucosa just lateral to the maxillary second molar. The submandibular duct (Wharton’s duct) empties next to the frenulum in the floor of the mouth. The sublingual glands excrete their saliva into many ducts and their number and size are variable, but all empty into the floor of the mouth.
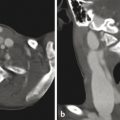
It is worth noting the various definitions and descriptions of the parapharyngeal space (Fig. 23.3). The parapharyngeal space is relatively large, extending from the angle of the mandible inferiorly to the skull base superiorly, bounded laterally by the masticator space, and bounded medially by the pharynx. Some textbooks refer to a fascial ligament from the styloid process to the tensor veli palatini, dividing the parapharyngeal space into the prestyloid (lateral) and poststyloid (posteromedial) spaces. The terms parotid space and carotid space are often used and essentially represent the prestyloid and poststyloid spaces, respectively.

A source of confusion is that neither the prestyloid nor poststyloid space contains the submucosal connective tissue and parapharyngeal fat pads. The submucosal space that contains these structures is also called the parapharyngeal space in some texts concerning the head and neck, and is also called this by oral and maxillofacial surgeons, and one can argue that this space is more deserving of the term “parapharyngeal space” because it surrounds the pharynx. However, given that this space is not included in the parapharyngeal spaces described above, these areas are referred to as the “pharyngeal submucosal space.” This submucosal space is very important for two reasons: (1) displacement of the fat in this space (seen on computed tomography [CT] and magnetic resonance imaging [MRI]) by lesions in the other parapharyngeal spaces can help determine the location and diagnostic identification of these lesions; and (2) this space is a pathway for the downward spread of odontogenic infections from the oral cavity into the neck and mediastinum.
Lesions in the prestyloid space are typically of salivary gland (parotid gland) origin. A small portion of the parotid gland often extends medially between the posterior border of the mandible and the styloid ligament (a space referred to the stylomandibular tunnel), and sometimes extends all the way up to the parapharyngeal fat. Lesions in the prestyloid space will displace the parapharyngeal fat pad anteromedially and the carotid artery posteriorly.
Lesions in the poststyloid space (carotid space) are often vascular lesions, paragangliomas, or neural lesions. Most neural lesions in the poststyloid space involve the vagus nerve, which is typically located posterior to the carotid artery. A lesion that displaces the carotid artery anteriorly or one that is located posterior to the styloid process and extends laterally and enters the poststyloid space narrows the differential diagnosis to lesions arising in the poststyloid space.
The retropharyngeal space (part of the submucosal pharyngeal space) lies between the prevertebral fascia and the visceral fascia of the neck (see Chapter 17) and extends inferiorly into the mediastinum, serving as a pathway through which oropharyngeal infections can spread and cause mediastinitis.
23.3 Salivary Glands
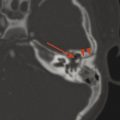
Primary neoplasms of the salivary glands are rare in children, although capillary hemangiomas of infancy can be associated with the parotid gland. Infection adjacent to a salivary gland can lead to secondary inflammation. Stones within the ducts of the salivary glands (sialoliths) increase the risk of sialadenitis.
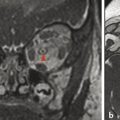
The ducts of the sublingual gland can become damaged and leak salivary fluid into the submucosa. A leaking salivary duct eventually becomes walled off by connective tissue, forming a pseudocyst termed a mucocele. When this occurs in the floor of the mouth, the mucocele is known as a ranula, and will be hyperintense on T2 W imaging, show no central enhancement, and have a thin peripheral wall without focal nodularity. A ranula can be confined to the sublingual space or can have cervical extension by coursing posterior to the mylohyoid muscle (or through a congenital defect in the myelohyoid); this is known as a plunging (or diving) ranula, and will nearly always be located lateral to the midline. 1 A midline cystic lesion in the floor of the mouth, typically in the posterior base of the tongue, is more likely to be a thyroglossal duct cyst (Fig. 17.4), which is discussed in Chapter 17. 2
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


