3 Asymmetry of the Lateral Ventricles
3.1 Case Presentation
3.1.1 History and Physical Examination
A 59-year-old male presented with headaches. The neurological examination was unremarkable.
3.1.2 Imaging Findings and Impression
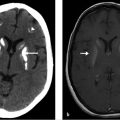
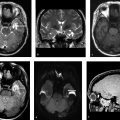
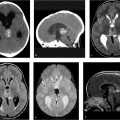
Axial (▶ Fig. 3.1a) and coronal (▶ Fig. 3.1b) images from a noncontrast head CT show asymmetry of the frontal horns (white arrows) of the lateral ventricles. There was no dilatation of the temporal horns (not shown).

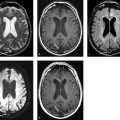
Axial T2-weighted imaging (T2WI; ▶ Fig. 3.2a) and fluid-attenuated inversion recovery (FLAIR) weighted imaging (▶ Fig. 3.2b) of the brain without contrast show asymmetrical prominence of the right lateral ventricle as compared to the opposite side (black arrows). The temporal horns were normal in size and there is no evidence of transependymal flow of cerebrospinal fluid (CSF) to suggest hydrocephalus (▶ Fig. 3.2c).

3.2 Differential Diagnosis
Asymmetric lateral ventricles:
Minimal asymmetry of the lateral ventricles, involving the frontal horns without signs of transependymal flow or mass involving the foramen of Monro.
Unilateral obstructive hydrocephalus:
The degree of asymmetry is typically more severe.
Associated with periventricular edema or transependymal flow of CSF.
An intraventricular or periventricular lesion may be causing obstruction of one foramen of Monro.
Causes may include the following:
Adhesion/synechiae post infectious ventriculitis or hemorrhage.
Congenital atresia.
Choroid plexus lesion.
Cysts: colloid cysts, neurocysticercosis, ependymal cysts, etc.
Tumor: subependymal giant cell astrocytoma (SEGA).
Vascular malformations.
High-resolution, multiplanar 3D sequences and heavily T2WI that are immune to CSF flow artifact have better specificity as they are able to directly visualize the foramina and look to see if there is a mass causing obstruction.
When questions remain, CSF flow studies can be performed to see if there is evidence of normal flow through the foramen of Monro, thus supporting the diagnosis of a normal variant, lateral ventricular asymmetry.
Ipsilateral atrophy due to encephalomalacia (Dyke–Davidoff–Masson syndrome):
Ipsilateral dilatation of ventricle secondary to atrophy of the brain.
Associated hypertrophy of calvarium and sinuses on the ipsilateral side.
Ipsilateral hemimegalencephaly:
Congenital malformation with defective cellular organization/migration.
Presence of polymicrogyria/lissencephaly/pachygyria ipsilateral to dilatation of ventricle.
Ipsilateral thickened calvarium.
Contralateral extrinsic mass effect.
Herniation syndromes leading to compression of the foramen of Monro, post shunting.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


