(1)
Department of Radiology Chair, Central State Medical Academy Department of Radiology, Moscow, Russia
3.1 Indications
In our view the main indication for ABVS should be dense breast tissue. In patients with fatty degeneration, the prevailing method is mammography.
ABVS should be used for supplemental screening after MMG in doubtful diagnostic cases or if masses or groups of microcalcifications were detected. When the lesion is evident on a mammogram, the topographic diagnosis is established with ABVS in relevant slices. Conversely, all local changes identified during ABVS could be projected on a mammogram, defining the characteristic radiographic features of the masses.
Reproducibility, the possibility of delayed interpretation, and second-look readings in automatic breast volume sonography provide unlimited opportunities for examiner-independent monitoring of benign masses.
A higher level of comfort for patients with breast implants is provided during ABVS examination compared to traditional mammography systems due to minimal breast compression during the study.
One of the major advantages of ABVS over other radiological methods (mammography and MRI) is that the images are produced with the patient in a supine position, similar to that for breast surgery. Therefore, the coronal slices can be used for surgical planning. These images are more easily interpreted not only by radiologists but also by surgeons.
Despite some difficulties in the scanning of patients with macromastia, we believe that this condition is also an indication for ABVS. Additional slices of the lower and mediolateral quadrants and special patient positioning during the examination allow the whole breast to be examined in macromastia cases.
To summarize, the indications for ABVS are the following:
Exclusion or confirmation of cancer signs in BI-RADS 3–5 lesions, detected by US or MMG in women with dense breast
As a screening method for young women with a high risk of breast cancer
Documentation of multifocality or multicentricity of BI-RADS 5 and 6 tumors
To follow up benign tumors
Postoperatively to identify the glandular structure
To clarify the topography of masses before biopsy or surgery
The potential indications for a more expanded ABVS study could be detection of cancer in young patients with a high risk of breast cancer, detection of multicentricity and multifocality of tumors (especially DCIS), study of the contralateral breast with existing breast cancer (in a hereditary disease, the risk of contralateral breast cancer reaches 65 %), detection of a residual tumor after lumpectomy, identification of occult breast cancer (when regional or distant metastases were found, in cases of MMG-negative or HHUS-negative tumors), precise estimation of tumor size (in a radiographically dense breast, in lobular carcinoma, in tumors with an extensive intraductal component, or, DCIS, if a lesion spreads in the surrounding tissue), and follow-up of the tumor during neoadjuvant chemotherapy before surgery.
Currently, the precise definition of the indications and risk groups for clinically and economically justified use of ABVS remains unclear. Also the screening interval for this group of patients and the optimal screening starting age are yet to be determined.
3.2 Technical Background
The ACUSON S2000 ABVS is an ultrasound system that includes an ultrasound scanner and a special stationary device with transducer attached to a mechanical arm (Fig. 3.1). The 14L5BV transducer (maximum frequency 14 MHz, average scanning frequency 10 MHz, width of 15.4 cm, 768 piezoelectric elements) receives the image of the entire breast volume in 1 min with a maximum depth of up to 6 cm. During the automatic collection of 3D data, 16.8 cm distance is covered, acquiring 318 high-resolution slices for post-processing (resolution: axial 0.09 mm, lateral 0.16 mm, and sagittal 0.44 mm).

Fig. 3.1
US device for automated breast scanning. ACUSON S2000 ABVS
In order to optimize the ABVS results, there is a wide range of known imaging modes including tissue harmonic imaging (THI), AdvancedSieClear™ spatial compounding, and Dynamic TCE™ (tissue contrast enhancement) technology, as well as new processing algorithms for nipple shadow and reverberation artifacts that are automatically applied when using the ABVS. The reverberation removal algorithm processes the 3D data and determines whether tissue contact is present and where it is not. The data corresponding to the area with no tissue contact are removed. This is intended to suppress reverberation artifacts from the noncontact areas. The adaptive nipple shadow reduction tool analyzes data on a case-by-case basis and is thought to enhance the structures in the retroareolar area and to improve visualization of this important region. And finally, a gain collection algorithm analyzes the 3D data and adjusts for the brightness variation artifacts caused by transducer channel-to-channel effects.
A replaceable membrane is fixed to the transducer to ensure sufficient contact with the skin of the entire area. The patient is placed in the same position as for the HHUS. A special lotion that provides optimal imaging results is applied to the skin instead of the usual gel (Polysonic Ultrasound Lotion, Parker Laboratories, Inc, Fairfield, NJ). The transducer is positioned on the breast with slight pressure and locked prior to scanning (Fig. 3.2).

Fig. 3.2
Special linear transducer (14L5BV) for automatic volume scanning
The depth of scanning is specified from A to D (depending on the bra cup size), and then the scan area is selected: the right or the left breast (Fig. 3.3). The transducer is positioned on the breast according to the selected slices (R AP, R LAT, R MED, R SUP, R INF, R AXILLA, R OTHER or L AP, L LAT, L MED, L SUP, L INF, L AXILLA, L OTHER, corresponding to the ROI) as anterior-posterior, medial, lateral, upper, lower, axillary, and other, according to the proposed positions (Fig. 3.4).


Fig. 3.3
The scanning parameters on the screen: depth, breast bra cup size, slice type
Fig. 3.4
The predefined positions of the scanner, with the number of standard slices for automatic scanning
Next, the scanning direction of the probe is selected by the button located on the transducer. The gathering of volume information may be performed upward or downward. Next stage is the acquisition of the 3D data. There is no need for the patient to hold her breath during the procedure. The probe is moved automatically in a given field, and at the end of the scan, it is automatically unlocked, so it can be removed from the gland. The automatic scanning procedure can be interrupted at any time by pressing the CANCEL button on the monitor screen.
3.3 Patient and Transducer Positions
We recommend the following special patient positioning for obtaining the ABVS slices.
3.3.1 AP Slice (Anteroposterior)
To obtain the slice, the patient is in a supine position with the ipsilateral hand behind the head. In this position the nipple is located centrally against the transducer where the arrow is, and the inner and outer quadrants of the breast are equidistant from it (Fig. 3.5). This is of major importance for precise further topographical measurements.

Fig. 3.5
Patient positioning and breast position while acquiring the coronal R AP slice. (a) Patient position during the ABVS study of the right breast. (b) Location of the breast under the transducer for an AP slice
3.3.2 LAT Slice (Latero-Medial Oblique (LMO))
The technique for obtaining the slice is similar to that of mammography, but the patient is lying on her side, with the ipsilateral hand behind her head. The nipple area is shifted medially as far as possible from the scanning field to the edge of the scanning membrane being equidistant from the upper and lower quadrants. The lateral scanning border of the transducer is marked with a red line (Fig. 3.6).

Fig. 3.6
Obtaining an R LAT slice (latero-medial oblique slice of the right breast). (a) Patient position during the ABVS exam. (b) Location of the breast under the transducer for an LMO slice
For the MED slice (mediolateral oblique (MLo)), the gland is shifted laterally to the side; the patient is in a supine position as during the AP slice with a maximum lateralization of the nipple in the scanning field (Fig. 3.7).

Fig. 3.7
Obtaining an R MED slice (mediolateral oblique slice of the right breast). Patient position
3.3.3 SUP Slice (Craniocaudal Superior-to-Inferior Slice)
To obtain this slice, it is necessary to raise the head of the couch in a slightly higher position with the ipsilateral arm lying close to the body. In severe breast ptosis, this maneuver is not needed. The transducer presses on the breast and shifts it downward to the chest. The nipple area in this position is displaced down from the scanning field, 1 cm from the membrane, centrally, so that inner and outer quadrants should be equidistant from the nipple (Fig. 3.8).

Fig. 3.8
Obtaining the R SUP (craniocaudal superior-to-inferior slice of the right breast). Patient position
The INF slice (craniocaudal inferior-to-superior slice) is produced in the supine position, with the ipsilateral hand behind the head. The breast is shifted upward; the nipple is maximally displaced up the scanning membrane, 1 cm from the edge of the scanning field.
Maximum lateralization of the nipple in the mediolateral oblique (MED) or latero-medial oblique (LAT) and craniocaudal inferior-to-superior (INF) slices is applied to improve the visualization of the zone behind the nipple. If the lesions are located in the inner quadrant or in the lower quadrant, it is preferable to use the MED or INF slices instead of LAT or craniocaudal superior-to-inferior (SUP), respectively.
A pictogram of the performed slice is presented in the lower-left corner of the screen. This stage is used for selection of the best quality ABVS image series for storage. At this stage, the quantity, quality of the acquired information, adequacy, and necessity of additional scans are verified. It should be noted that the assessment of the quality of sonotomograms is important at this stage, as the patient is still in the examination room and the breast can be re-scanned with additional slices if necessary. During an automatic scan, motional or conversation artifacts arise in some cases, which adversely affect the perception of 3D data. Therefore, during the automatic scanning, the patient should not talk or move. Breathing chest movements do not interfere with scanning and do not alter the image. The lack of contact of the scanning membrane with the skin of the gland can cause some so-called “dark side” artifacts; this should be avoided. Unfortunately, it is difficult to achieve in some cases, e.g., in patients with breast scar deformation after breast conserving surgery or lumpectomy, in breast-expanders, in large tumors with nipple retraction, or, vice versa, with the bulging of the mass and, less often, after breast augmentation.
If the operator is satisfied with the information collected, he/she labels the position of the nipple, which allows orientation in the subsequent analysis, and confirms the saving of the collected information by pressing the SAVE button, and then all the data are stored. When the image is of poor quality, no saving is performed by clicking the REJECT button.
After the first slice, the US device automatically offers to acquire the next one, as programmed in the presets of the US scanner. On average, six standard slices are performed per patient. According to our recommendations for the use of the technology, it is necessary to perform the coronal, oblique latero-medial (or mediolateral), and craniocaudal superior-to-inferior slices of each gland. The number of slices depends on the size of the breast. The larger the breast, the more slices you need to perform. The more masses are examined; the more slices should be performed to fully collect all the information.
3.4 Image Analysis
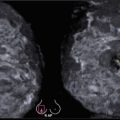
After a particular scan is completed, the coronal plane of the acquired volume is displayed at skin level. This information is presented on the screen as a series of images that can be resliced from the top with the nipple down to the chest wall. The per-quadrant anatomy on ABVS scans corresponds to the real location of the quadrants in the breast. The upper quadrants in all images using this technology are at the top of the scan, and the outer and inner quadrants correspond to the patient’s position during the examination (Fig. 3.9).

Fig. 3.9
US tomograms performed according to the technology under our recommendations. Right breast, three images; left breast, three images. Symbols: R-CC, right SUP slice; L-CC, left SUP slice; R AP, right anteroposterior coronal slice; L AP, left anteroposterior coronal slice; R-ML, right MED slice; and L-ML, left MED slice
Before collecting the next slice, quick preliminary topographical measurements could be performed for the entire volume produced on the screen. The image can be analyzed quickly by activating the Advanced 3D function on the monitor screen. It opens an extended menu for analysis of three-dimensional information. The most commonly used is two-view mapping mode. When an unclear object is selected on a cross section, the second part of the screen displays its coronal view. The left part of the screen shows the standard cross-sectional view of the mass of interest, and the right part of the screen shows the matching coronal slice (Fig. 3.10). Multislice analysis of the tumor can also be performed by specifying the slice thickness and desired plane. The US device allows the operator to set the required number of images on the screen during multislice viewing (Fig. 3.11). A cross-sectional view can be combined with multislice technology and provides data on a single picture (Fig. 3.12). The distance from the mass to the nipple, from the mass to the skin, or from the mass to the chest wall can also be measured. The entire breast structure is evaluated on the cine view; localization of lesions is clarified for quick appreciation of the pathology. There are plenty of choices for analysis of 3D data stored in the device.