4 SPECT/CT for the Thyroid and Parathyroid Glands with Cases
4.1 Introduction
Single-photon emission computed tomography/ computed tomography (SPECT/CT) has substantially improved patient care in the management of several endocrine disorders previously managed with planar imaging or with planar imaging and SPECT together. Before the advent of hybrid imaging systems (positron emission tomography [PET]/ CT and SPECT/CT), the CT images were collected separately from the planar or nuclear tomographic images, and the interpreting physician would look at the separate image sets and make a best guess at the “fusion” of the data sets. In some cases, the fusion was relatively easy to observe, such as when a solitary pulmonary nodule was found on CT and determined to be the same size and at the same location as a solitary focal concentration of tracer seen on fluorodeoxyglucose (FDG)-PET images. In many endocrine cases, however, lesions are small and often adjacent to structures that normally concentrate tracer, such as the gastrointestinal (GI) tract or salivary glands. Differentiating normal activity from abnormal activity then becomes a bigger challenge, particularly in postsurgical patients. As with FDG-PET/CT in patients with other malignant disease, SPECT/CT has drastically reduced the difficulty of fusing anatomical and physiological data sets obtained at different time points, improving the accuracy of tracer localization in many patients with thyroid and parathyroid neoplastic disease.
Pearls and pitfalls of SPECT/CT include the following:
Tracer uptake may be faint and require additional time for SPECT data acquisition.
Small focal sites of tracer uptake near the diaphragm may be subject to motion artifact, making localization more difficult or blurring the activity such that it cannot be seen at all.
In the thyroid bed, artifact from intense iodine-131 (131I) uptake following a therapeutic dose may render identification of adjacent nodal uptake difficult.
If diffuse uptake of radioiodine is seen in the lung and the CT scan shows no anatomical signs of metastasis, the iodine uptake is still most likely secondary to metastatic thyroid disease.
Posttherapy radioiodine imaging is more sensitive (and specific) for metastatic spread of thyroid cancer to the lungs than noncontrast chest CT and chest X-ray. 1 , 2 , 3 , 4
4.2 For Benign Thyroid Disease
SPECT/CT is not often used for benign thyroid conditions, such as Graves’ disease, thyroid nodules, or thyroiditis. If anatomical information is needed, a thyroid ultrasound is usually sufficient. Planar images with marker views of a palpable thyroid nodule can be correlated easily enough with ultrasound imaging. While SPECT/CT is not commonly used for benign thyroid disease, in some cases it can be helpful.
4.2.1 Case 1: Multinodular Goiter
History
A 76-year-old woman with known multinodular goiter and hyperthyroidism presented to her endocrinologist because a left thyroid nodule was increasing in size. Ultrasound showed multiple nodules bilaterally, with a cyst at the upper pole on the right. Because there was a question of the functional status of the enlarging nodule, a SPECT/ CT was performed.
Physical Examination
Physical examination revealed a markedly enlarged, nontender, partially substernal multinodular thyroid gland.
Imaging Findings
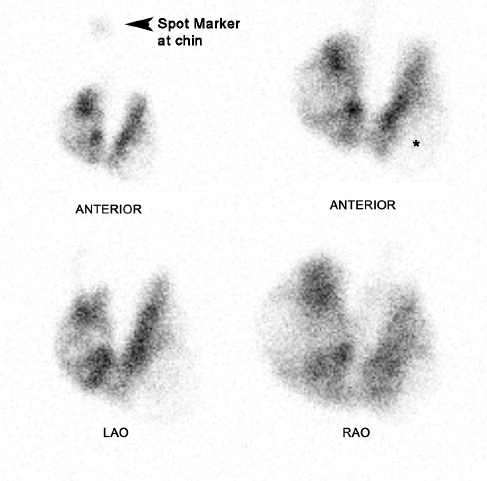
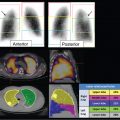
The 24-hour uptake of radioiodine (iodine-123 [123I]) was measured to be 40%. The planar images show an enlarged thyroid gland with heterogeneous iodine uptake (► Fig. 4.1). There are multiple areas with decreased tracer uptake and fewer areas with relatively increased tracer uptake. The biggest defect is noted in the left lower lobe (shown on the planar images).
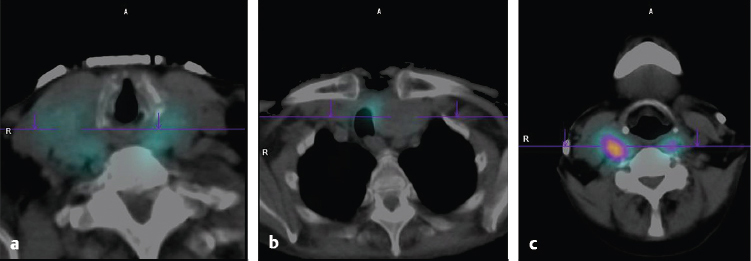
On SPECT/CT (► Fig. 4.2), the low-resolution CT of the SPECT/CT shows that most of the thyroid nodules have no iodine uptake. Sites of increased tracer uptake in the posterior, medial, and upper poles of both lobes correspond to thyroid tissue with no nodule (► Fig. 4.2 c).
Discussion/Diagnosis
In this case, focal uptake in the thyroid gland on planar scintigraphy raised the concern of a hyperfunctioning nodule, possibly contributing to the hyperthyroidism. SPECT/CT showed that the nodules seen on ultrasound did not take up tracer, while the sites of increased tracer uptake were associated with nonnodular thyroid tissue, consistent with Graves’ disease in a multinodular goiter.
Functioning nodules (showing iodine uptake) are so rarely associated with thyroid malignancy that they do not need biopsy. In addition, hyperfunctioning nodules can show distorted follicular architecture and therefore can be difficult to distinguish from neoplastic tissue upon histological examination. 5 , 6 , 7
The dominant cold nodule was biopsied, but the results of the histological examination are not available.
4.2.2 Case 2: Hyperfunctioning and Hypofunctioning Nodules
History
A 53-year-old woman presented with three nodules seen on ultrasound of the right thyroid lobe. The functional status of the nodules is being pursued. The thyroid-stimulating hormone is suppressed.
Physical Examination
Thyroid examination was difficult secondary to body habitus; however, palpation of the right thyroid lobe revealed it to be prominent with an irregular surface.
Imaging Findings
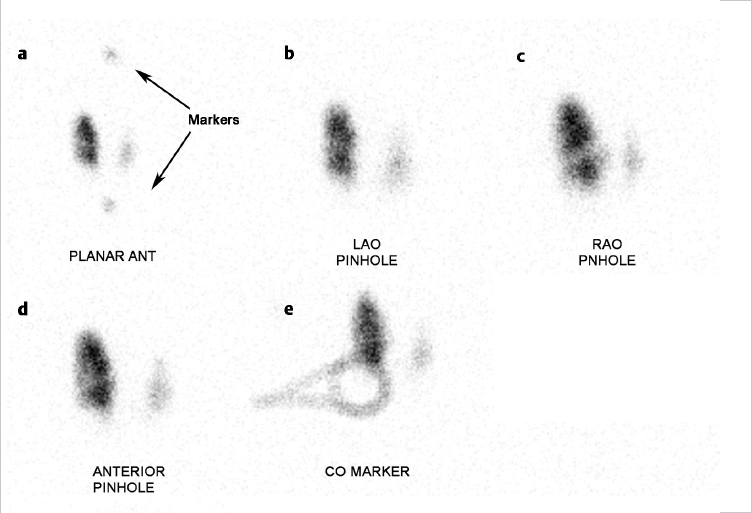
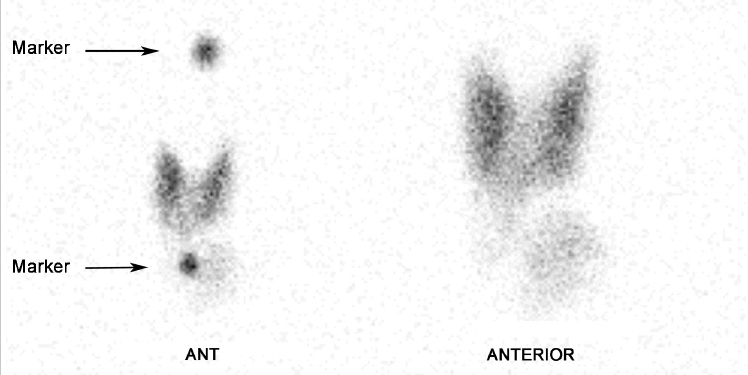
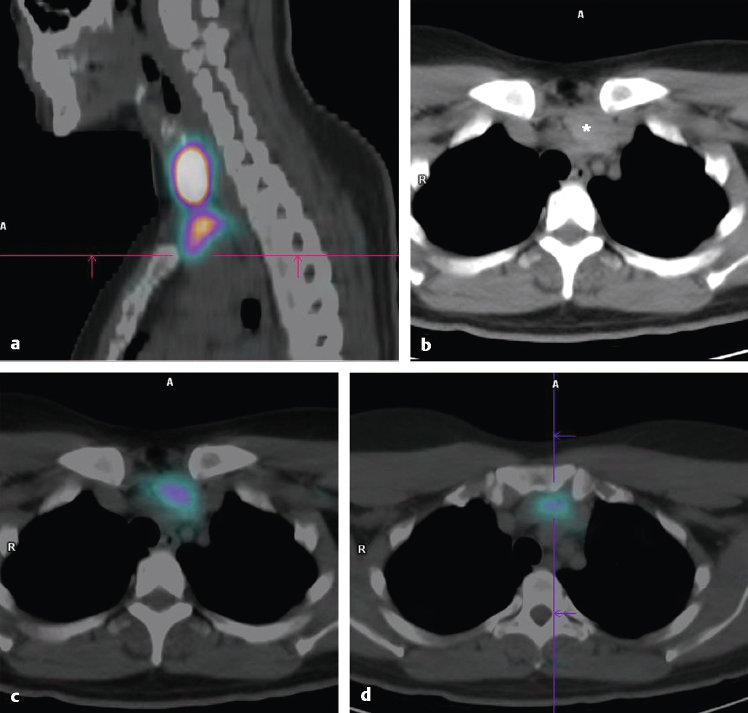
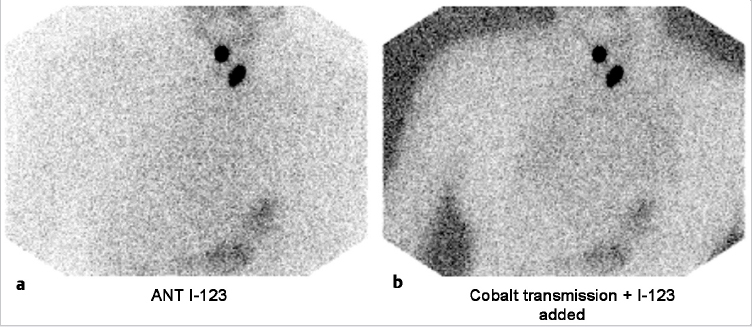
The 24-hour uptake of radioiodine was measured to be 22%. Planar images show irregular uptake throughout the thyroid gland with relatively increased tracer uptake on the right compared to the left. The dominant nodule on palpation was marked using a cobalt-57 string marker, which, on imaging, appeared to be placed over the lower pole of the right thyroid lobe in a region of minimal iodine uptake. Because there was difficulty palpating the thyroid gland, the correct placement of the marker over the dominant nodule was questioned (► Fig. 4.3).
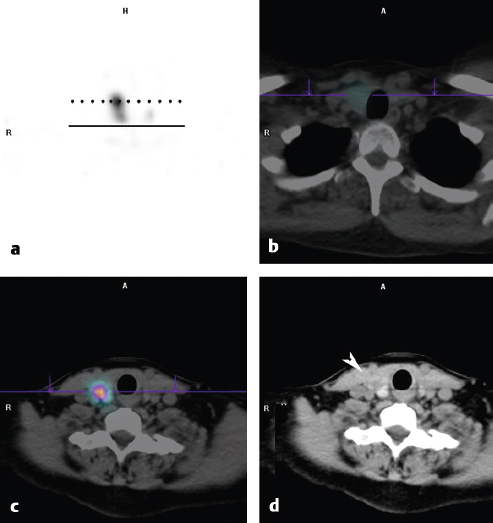
On SPECT/CT, the two sites of increased tracer uptake correspond to nodules in the upper pole and middle portion of the right thyroid lobe, and the inferior nodule shows no tracer uptake. The two relatively hyperfunctioning nodules are suppressing the function of the rest of the thyroid gland (► Fig. 4.4).
Discussion/Diagnosis
While correlation of ultrasound findings with physical examination and planar images with marker views is often adequate to determine the functional status of thyroid nodules, when physical examination is difficult and reliable placement of the marker is questioned, SPECT/CT can be very helpful. SPECT/CT, in this case, confirmed that the dominant nodule in the lower pole of the right thyroid lobe was nonfunctioning, while the two nodules in the right middle and upper thyroid lobe corresponded to hyperfunctioning nodules. The lower pole nodule was biopsied and found to be benign. The relatively hyperfunctioning nodules higher in the right thyroid lobe were suppressing tracer uptake in the left thyroid lobe.
Pearls
Hyperthyroidism associated with Graves’ disease usually results in an elevated 24-hour uptake of radioiodine in the thyroid gland; however, a hyperfunctioning nodule may not store as much iodine as the entire gland; therefore, whole-thyroid uptake measurements in glands with hyperfunctioning nodules can often be normal.
4.2.3 Case 3: Prominent Pyramidal Lobe
History
A 45-year-old woman presented with Graves’ disease. The patient gave a history of hyperthyroidism for approximately 10 years, treated with methimazole for the past 8 years. A prior scan at another institution showed an unusual contour of the right upper pole/pyramidal lobe region and raised a question of a hypofunctioning nodule versus a large medial pyramidal lobe. Ultrasound showed heterogeneous iodine uptake throughout the gland, with several small nodular regions. The largest nodule in the left lower pole was 1 cm. Biopsy of that nodule was negative.
Physical Examination
Physical examination revealed an enlarged, soft, nontender thyroid gland that is slightly irregular without clear nodules. Palpated tissue near the midline, in the expected location of the pyramidal lobe, was more prominent than usual.
Imaging Findings
The 24-hour uptake of radioiodine was measured to be 95%. There was misregistration of SPECT and CT data, but the thyroid gland, including the pyramidal lobe, can be detected by increased attenuation on CT. There is no focal area of decreased tracer uptake that correlates with the expected location of the thyroid nodule. The pyramidal lobe shows tracer uptake (► Fig. 4.5).
Discussion/Diagnosis
This is an unusual case in which the pyramidal lobe of a hyperfunctioning gland made correlation of ultrasound, physical exam, and planar imaging difficult. SPECT/CT was helpful to show that the defect on the planar images did not correspond to the nodule seen on ultrasound. The final diagnosis was Graves’ disease with a prominent pyramidal lobe.
Pearls
When viewing hybrid imaging studies (PET/CT and SPECT/CT), the possibility of misregistration between the CT and the scintigraphic data should always be considered, particularly when small structures are being evaluated. Determining if misregistration has occurred can be particularly difficult with thyroid imaging using radioiodine because of the lack of tracer uptake in adjacent landmarks.
4.2.4 Case 4: Ectopic Thyroid Tissue
History
A 27-year-old man presented with hypothyroidism. No thyroid tissue was seen on ultrasound.
Physical Examination
No thyroid tissue was palpated.
Imaging Findings
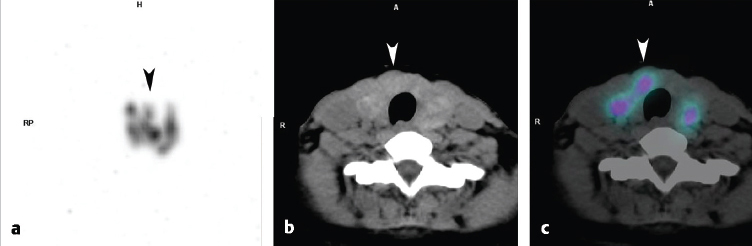
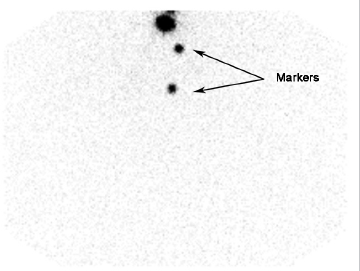
Planar images show no tracer uptake in the region of the thyroid bed; however, focal uptake is seen high in the neck (► Fig. 4.6). SPECT/CT showed that the site of tracer uptake was at the base of the tongue on the right (► Fig. 4.7). Visual examination of the base of the tongue showed evidence of a very small rest of lingual thyroid tissue on the right.
Discussion/Diagnosis
SPECT/CT is very useful for distinguishing functioning ectopic tissue from adjacent structures that can normally show iodine concentration, such as salivary glands, collections of saliva in the mouth, and swallowed saliva in the esophagus.
Pearls
Ectopic thyroid tissue typically does not function normally, nor is it the same size as a normal thyroid gland; therefore, measurement of 24-hour uptake of radioiodine cannot be compared to normal values and is not helpful for patient management. 8
4.2.5 Case 5: Retrosternal Goiter
History
A 50-year-old woman presented with a mediastinal mass incidentally discovered on CT scan.
Physical Examination
Thyroid function tests were normal. The thyroid was normal on palpation except for evidence of ullness inferiorly.
Imaging Findings
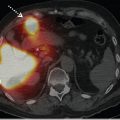
The thyroid planar images (► Fig. 4.8) and SPECT/ CT (► Fig. 4.9) demonstrated uptake of iodine within the mass, therefore confirming the presence of thyroid tissue. Histological sampling was unsuccessful, and the mass was removed by partial thyroidectomy.
Discussion/Diagnosis
Tissue masses just inferior to the thyroid gland in the anterior mediastinum may be suspected to be thyroid tissue; however, the differential diagnosis includes a number of neoplasms, and a tissue diagnosis is needed, particularly if the mass is causing symptoms such as shortness of breath or dysphagia due to airway or esophageal obstruction. Imaging with 123I or 131I can be helpful for confirming the presence of thyroid tissue. Substernal thyroid tissue often does not function normally, and iodine uptake may be diminished compared to uptake in normal thyroid tissue, as in this case. Pathology demonstrated the mass to be multinodular thyroid tissue.
Pearls
The four most common causes of anterior mediastinal masses can be remembered as the “four Ts”:
Teratoma/germ cell tumor.
Thymoma.
Thyroid tissue.
Terrible lymphoma.
4.3 For Thyroid Cancer
According to the American Cancer Society, approximately 60,000 thyroid cancers occurred in the United States in 2014, yet in that same year there were fewer than 2,000 deaths from thyroid cancer. The indolent nature of the disease is partly responsible for the low mortality; however, the incidence of thyroid cancer is increasing more rapidly than any other malignancy in the United States. Part of this increase in incidence may be attributable to the practice of head and neck irradiation, which occurred more commonly in the first half of the 20th century to treat skin diseases in children. More recently, much of the increase is thought to be secondary to the increased utilization of neck imaging, such as ultrasound, and the ease of histological sampling with fine-needle aspiration. 9 , 10 , 11 , 12
While the indolent nature of the disease helps to keep the mortality low, proper staging of the disease remains important because patients with stage III and stage IV disease have increased mortality, albeit with evidence of prolonged life span following 131I therapy. 13 , 14 , 15 Staging of thyroid cancer is usually based on the TNM (tumor, node, metastasis) system. 1 , 16 SPECT/CT can be an important tool for improving specificity over planar imaging for the diagnosis of metastatic disease, as well as improving sensitivity for nodal disease in the region of the thyroid bed. 13 , 17 , 18 , 19
In the thyroid bed, SPECT/CT following thyroid surgery is helpful for separating local nodal uptake from remnant thyroid tissue. Local nodal disease, particularly outside the thyroid bed, may be treated more aggressively than remnant thyroid tissue alone. 20 , 21 Focal tracer uptake at a distant site of disease in the chest, abdomen, or pelvis may also be more easily found using SPECT/CT. Sites of metastatic tracer uptake distant to the thyroid gland can be confused with normal structures, such as tracer normally found in the urinary collecting system or GI tract. In some cases, uptake in the region of the diaphragm seen on planar images can be either in the lungs or normal tracer concentration in the bowel or kidneys.
Identification of the cause and location of focal tracer uptake can be helpful in the initial staging of patients with thyroid cancer and at the time of subsequent visits as well.
4.3.1 Case 6: Thyroid Bed Uptake
History
A 74-year-old man presented with follicular variant papillary thyroid cancer.
Physical Examination
Physical examination was not performed.
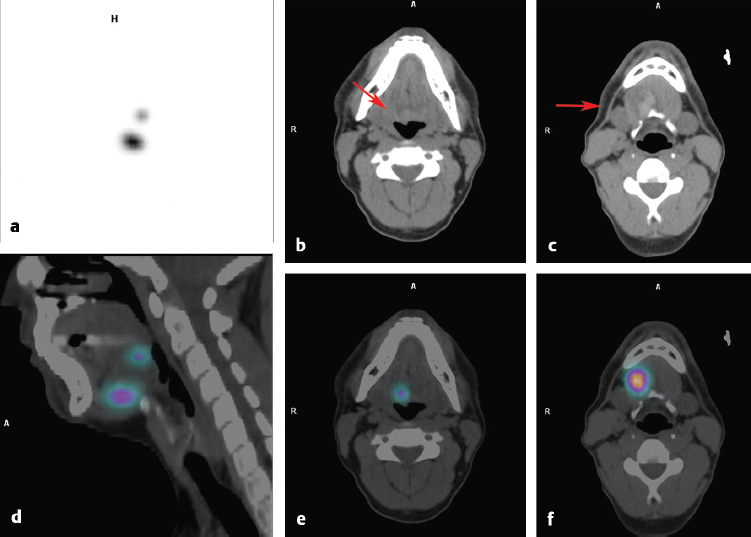
Imaging Findings
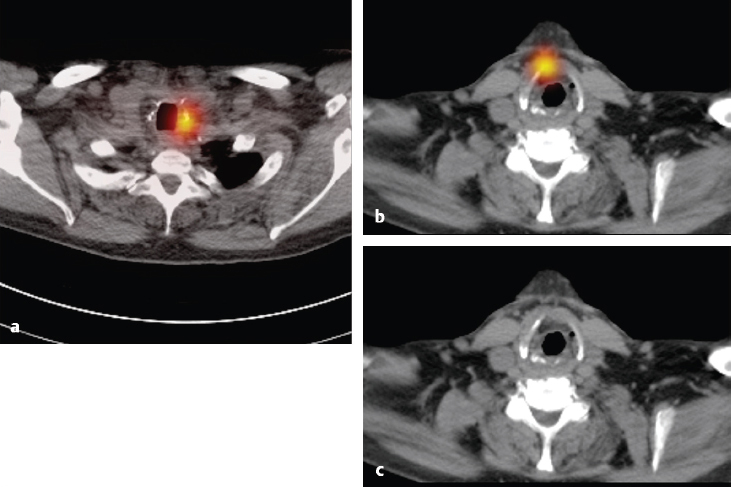
123I planar images (► Fig. 4.10) show sites of tracer uptake in the base of the neck. There was a question as to the exact location of the uptake, and SPECT/CT was performed. SPECT/CT images show focal uptake in the left thyroid bed (► Fig. 4.11 a) and anterior to the trachea (► Fig. 4.11 b, c), consistent with a thyroglossal duct remnant.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


