6 Lung Ablation (Part I)
Percutaneous thermal tumor ablation (PTTA) is a minimally invasive treatment alternative for primary and secondary pulmonary malignancies. Thus far, the majority of ablative technologies focus on thermal, chemical, and cell permeability techniques, of which thermal energy has been the most studied and widely used in the thorax and lung. Thermal energy sources can be heat-based (radiofrequency and microwave) or cold-based (cryoablation). To date, radiofrequency ablation (RFA) has been the best developed, although continued advances in microwave and cryoablation technologies have led to their increased utilization and investigation with newly emerging technology-specific benefits.1,2 The emergence of more fully realized thermal ablative technologies, in culmination with image-guided, or minimally invasive, approaches, offers a valuable alternative, or at a minimum, a useful adjunct to conventional or limited surgical resection.
The indications for thermal ablation in the thorax as a standalone technique or in combination with other therapeutic options include stage 1 and 2 non-small cell lung cancer (NSCLC) both medically operable and inoperable candidates, carefully selected stage 3a NSCLC, reduction or debulking of tumor burden in anticipation of limiting vital structure involvement or enhancing eligibility for later resection, control of limited recurrent or metastatic disease, and palliation for pain control.
With refinements in technology, patient selection, clinical applications, and methods for follow-up, PTTA will continue to flourish, as a viable stand-alone or complementary therapy for both primary and secondary lung malignancies in standard and high-risk populations.
♦ Current Treatment Options and the Role of Ablation
The treatment of primary and secondary pulmonary malignancies has evolved into a multidisciplinary approach allowing for combination therapies and the use of novel chemotherapeutic agents, targeted radiotherapy, and thermal ablation. An overview of the current treatment options for primary and secondary pulmonary malignancies in the medically operable and inoperable patient is necessary to understand the role and benefit of percutaneous thermal ablation in relation to other treatment options.
Treatment options for NSCLC are multifactorial but based primarily on the stage and medical fitness of the patient. In stage 1 (tumor, node, metastasis [TNM] stages T1 N0 M0 and T2 N0 M0) and stage 2 disease (T1 N1 M0, T2 N1 M0 and T3 N0 M0), surgery is the treatment of choice with a 5-year survival of approximately 75% and 50%, respectively.3 In stage 3a disease (T1 N2 M0, T2 N2 M0, T3 N1 M0, and T3 N2 M0), radiotherapy, chemotherapy, surgery, and combinations of these modalities are used for treatment, with an overall 5-year survival that does not exceed 10 to 15%.3 In stage 3b disease (any T, N3, M0 and T4, any N, M0), surgery is of no benefit. A combination of chemotherapy and radiotherapy is used with a 5-year survival of less than 5%.3 In stage 4 disease (any T, any N, M1), palliative chemotherapy is used with a median survival at the time of diagnosis of only 7.9 months.4 Although surgery is the preferred method for stage 1 and 2 NSCLC,5 only one third of these patients meet pulmonary physiologic guidelines for lobar or sublobar resection (forced expiratory volume in 1 second [FEV1] >60% predicted and carbon monoxide diffusing capacity of the lungs [DLCO] >60% predicted).6 According to the Surveillance, Epidemiology, and End Results (SEER) database, 14,555 patients, or 15.7%, present with stage 1 and 2 lung cancer but are medically inoperable.7 For these candidates, sublobar resection, specifically wedge resection and segmentectomy, has been proposed, but because of its higher local recurrence rates compared with traditional lobectomy of up to 50%, sublobar resection is considered less favorable and has been viewed by many as a compromised operation.8 Despite comorbid medical illness, however, candidates who receive some form of therapy for early-stage lung cancer demonstrate better outcomes than those who do not receive any form of therapy.9 Therefore, a sizable proportion of patients with stage 1 and 2 lung cancer are medically inoperable and can benefit from less invasive and nonsurgical alternatives, such as percutaneous thermal tumor ablation.
Thermal ablation, in combination with radiation or chemotherapy, for inoperable candidates is being pursued and appears intuitive. Candidates who have been treated with combination therapy include those with limited local recurrence after enjoying a period of remission following chemotherapy and/or radiation and those with large initial tumor bulk, usually more than 3 cm, or tumor within a precarious location to vital structures, especially compelling for the use of combination therapy. Comparatively, conventional radiation alone in inoperable early-stage NSCLC has shown survival rates of approximately 30% at 5 years,10,11 although newer advances in radiation therapy, particularly stereotac-tic body radiotherapy offering highly focused and precise delivery of a higher biologically effective dose than conventional radiation, have shown promising results but have not yet gained widespread availability.12–14
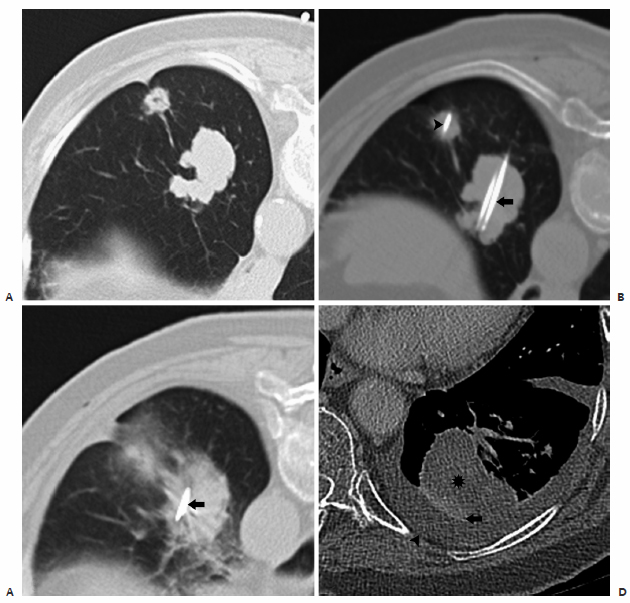
In patients with NSCLC, radiofrequency ablation and radiotherapy are synergistic. A proposed mechanism is believed to be that RFA has a greater effect in the central portion of the tumor, which often contains areas of diminished oxygenation and therefore is less responsive to radiotherapy, and a lesser effect in the peripheral portion tumor with a surrounding zone of nonlethal heat injury that increases sensitivity to external-beam radiation.15 With the synergism of combined therapy, potential cure may be offered for larger tumors than with RFA alone ( Fig. 6.1 ). Grieco and colleagues15 reported results for patients after thermal ablation (either RFA or microwave ablation) followed by radiation therapy (either external-beam radiation or interstitial brachytherapy) for stage 1 or 2 NSCLC. Overall survival rates were 86.8%, 70.4%, and 57.1% for 1, 2, and 3 years, respectively. Similar to earlier experiences, the reported survival rates for combination therapy were higher than those seen with RFA alone.15–17 Interestingly, the survival rates were similar for stage 1a and 1b, suggesting that radiotherapy may improve the efficacy of thermal ablation for the treatment of larger tumors ( Fig. 6.1 ). However, and perhaps somewhat discouragingly, local recurrence remained higher in tumors larger than 3 cm.15
In regard to adjuvant therapy, cisplatin-based chemotherapy has demonstrated a survival benefit in patients with stage 2 disease and higher.18 However, no significant improvement in survival was seen in stage 1b disease, with a negative effect observed in patients with stage 1a disease, and up to 50% of patients with stage 1b NSCLC eventually develop disease recurrence despite initial treatment with curative intent.18 Chemotherapy alone is not indicated for early-stage lung cancer and should be accompanied with surgical resection or thermal ablation. Similarly, thermal ablation for early-stage lung cancer should be accompanied by adjuvant chemotherapy for better survival.
In small cell lung cancer (SCLC), treatment is based on the extent of disease, with surgery being of no benefit for extensive disease. Extensive stage SCLC is treated with combination chemotherapy, with radiotherapy alone demonstrating no significant benefit. In limited-stage disease, combination chemotherapy is the cornerstone of treatment and is typically combined with radiotherapy with a median survival of 18 to 24 months and a 2-year survival of 40 to 50%.19,20 Surgery plays a limited role in stage 1 SCLC. Currently, the effects of thermal ablation in limited SCLC has not been investigated but, seemingly as surgery, potentially could be used to treat peripheral limited stage 1 SCLC.21
Metastatic disease by solid tumors to the lungs is common, with the lung being the second most commonly affected organ, following the lymphatic system.22,23 Hematogenous metastases from nongastrointestinal tumors to the lungs occur with reasonable frequency, as the lung acts as the first capillary bed for blood-borne and lymphatic-borne dissemination.24 Approximately 20% of candidates with lung metastases, who have already undergone resection of the primary soft tissue tumor, have a limited number of metastases located only within the lung, rendering them potential candidates for surgical resection, or metastasectomy.23 Surgical metastasectomy results in improved disease-free survival in properly selected patients, particularly in those with metastatic colorectal carcinomas and sarcomas.25–27 In contrast to primary lung carcinoma where lobar resections and pneumonectomy confer increased rates of survival, no difference in survival outcome between wedge and lobar resections and pneumonectomy was seen in the metastasectomy population; therefore, resection with the least amount of loss to lung parenchyma has been advocated.28–30 Notably, percutaneous thermal ablation, with its minimal invasiveness and ability to spare lung, is an attractive alternative for those patients with limited metas-tatic disease who are medically inoperable; have limited recurrent or residual disease following prior surgical resection, chemotherapy, or radiotherapy; or deemed surgically inoperable from decreased lung volumes or pleural adhesions.
In simplistic terms, percutaneous ablation can be reasonably considered in those patients with surgical disease, whether primary or secondary malignancy, who are, for one reason or another, medically or surgically ineligible. The treatment of primary and secondary pulmonary malignancies in the inoperable patient will continue to evolve, with the role of thermal ablation being better defined as increasing long-term data emerges. It is clear that a multidisciplinary, or “team,” approach individualizing therapy to each patient’s disease will be the standard going forward, with thermal ablation being used as a monotherapy, or in combination with surgical resection, radiotherapy, and/or systemic therapy in carefully selected patients.
♦ Patient Selection, Tumor Selection, and Anatomic Considerations
Proper patient selection for PTTA is highly dependent on the anticipated goal to be achieved, with the understanding that thermal ablation provides only local control of cancer. Clinical indications, contraindications, and selection criteria are assessed together when evaluating patients for thermal ablation. Clinical indications are detailed in the previous section and principally include primary or secondary pulmonary or pleural malignancies, in which local control of tumor with and without curative intent as in debulking, reduction of total body tumor burden, or palliation of tumor and its effects is desired and sensible.
Pearls: Indications
Primary stage 1 or 2 lung cancer in medically inoperable tumors
Secondary pulmonary malignancies in particular with limited colorectal and sarcoma metastasis
Secondary pleural malignancies for local control with and without curative intent
There are few absolute and relative contraindications for thermal ablation, and, as a general rule, a patient who can undergo an image-guided biopsy can be considered a candidate for thermal ablation. Absolute contraindications, however, include severe pulmonary arterial hypertension (>40 mm Hg) and acute pneumonia. Relative contraindications include the inability to cooperate (lie flat and breath-hold), although rectified with general anesthesia and deep sedation; coagulation disorders/ medications; pacemakers/automatic implantable cardioverter-defibrillators (AICDs); and pneumonectomy, although some authors believe that thermal ablation can be safely performed even in this population if the proper preparations are made for rapid chest tube insertion.31,32
Although no strict criteria exist for patient selection, the emerging goals for ablation thus far established within the current literature include the potential for cure, prolongation of survival, and palliative relief of symptoms.
Candidates for whom there is a potential for cure include those with stage 1 or 2 NSCLC who are medically inoperable or refuse surgical resection, and those with limited or low-volume and indolent metastatic cancer from an extra-pulmonary primary malignancy, provided that the primary tumor site or extrathoracic sites of tumor are controlled. Candidates for whom there is a potential for prolongation of survival include those with pulmonary malignancy with limited disease outside the lung that can be treated with systemic therapy or locoregional methods, slowly growing pulmonary malignancy with the main bulk of tumor within the lung, and larger tumors where cytoreduction can alter the susceptibility of viable tumor tissue to chemotherapy or radiotherapy. Candidates for whom there is a need for palliation include those with painful peripheral tumors invading the parietal pleura or chest wall, those with tumors adjacent to vital structures as a preemptive strike before invasion, and those requiring cytoreduction of tumor volume to result in reduction of symptoms.
Pearls: Contraindications
Absolute: severe pulmonary arterial hypertension and acute pneumonia
Relative: inability to cooperate (lie flat and breath-hold), coagulation disorders/medications, pacemakers/AICDs and pneumonectomy
General rule: A patient who can undergo an image-guided biopsy can be considered for thermal ablation.
As with patient selection, strict criteria are also lacking for tumor characteristics favorable for thermal ablation, although clear trends have emerged. The ideal lesion is a solitary tumor that is completely intraparenchymal and ≤3 cm; treating tumors of this size results in higher rates of complete necrosis and ultimately improved survival.17,33 The combination of radiofrequency and targeted radiation has shown improved survival, specifically in lesions >3 cm, and should be pursued.15 For pleural and chest wall lesions, the use of cryoablation instead of heat-based ablative techniques has shown less patient discomfort and complications.34
For patients with multifocal disease, a finite number of metastases at presentation is desirable, ideally less than six in total, although this is a somewhat arbitrary criterion that is loosely based on metastasectomy data showing diminishing gains with higher numbers of resections.35 Other important considerations regarding the target lesion include confinement within a single ablation zone, higher sphericity, and noncontiguity with the hilum, including large bronchi, pulmonary arteries and veins, or vital mediastinal structures, such as the trachea, esophagus, heart, aorta, and great arteries. If one is considering the use of radiofrequency energy, additional forethought regarding the potential for the heat-sink effect from adjacent pulmonary arteries and veins >3 mm36 or large bronchi37 is necessary to avoid incomplete or partial ablation. However, with advances in microwave and cryoablation technology, the heat-sink effect can be minimized or obviated altogether. The texture of the lesion can also be important, as extremely dense or fibrotic lesions may be mobile or demonstrate a “push-back” phenomenon described by Steinke et al,38 in which the shaft of the electrode is continually pushed back with attempted tine deployment.
Pearls: Ideal Tumor Characteristics
Solitary tumor that is completely intraparenchymal and <3 cm
In multifocal disease a finite number of metastases, ideally <6
confinement to single ablation zone
Noncontiguity with the hilum and mediastinum
♦ Anatomic Considerations for Thoracic Ablation
Multiple anatomic factors should be taken into account when developing an approach for a percutaneous CT-guided pulmonary ablation. Similar to percutaneous CT-guided lung biopsy, site of entry, adequate pleural anesthesia, and awareness of the bronchovascular planes, the fissures, and the mediastinal structures is critical in maximizing patient comfort and increasing the success of the ablation while minimizing the risk for significant complications.
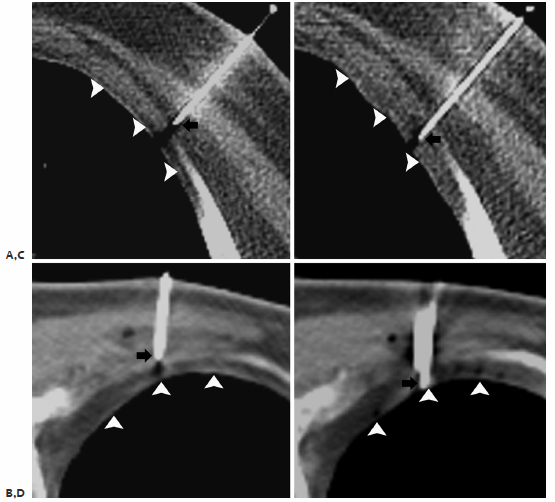
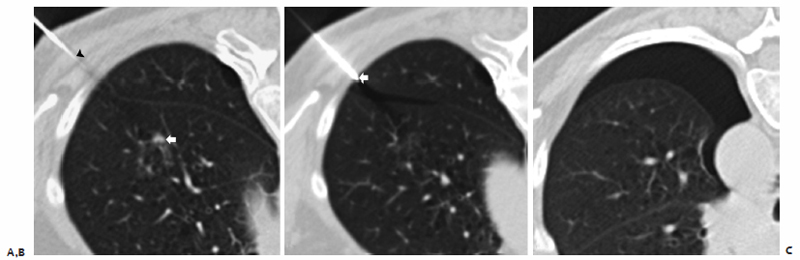
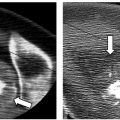
Initial adequate placement of the coaxial needle is essential for achieving pleural anesthesia and optimal trajectory for tandem placement of ablation electrode. Adequate pleu-ral anesthesia is the cornerstone of successful ablation, as patient comfort and cooperation are of the utmost importance. The parietal pleural is the second most sensitive structure aside from the skin in the path of the ablation electrode. The costal and diaphragmatic parietal pleura is innervated by the overlying intercostal nerve, where inadequate anesthesia is characterized by significant pain and discomfort along the dermatome or referred pain to the ipsilateral shoulder. Effective anesthesia of the parietal pleura requires the precise placement of the anesthesia needle tip in an extrapleural location immediately adjacent to and superficial to the parietal pleura, while avoiding both the underlying parietal and visceral pleura, which if violated increases the risk of pneumothorax ( Fig. 6.2 ). Proper needle tip placement requires the combination of exact measurements obtained from localization scans and operator needle control. As the needle penetrates the different layers of the chest wall, the operator will feel many “pops,” representing the needle traversing the different chest wall structures, the most important of which is the endothoracic fascia as its passages signifies the exact location of the extrapleural fat space immediately superficial to the parietal pleura, where a few millimeters can mean the difference between a straightforward ablation versus one complicated by a premature pneumothorax ( Fig. 6.3 ).
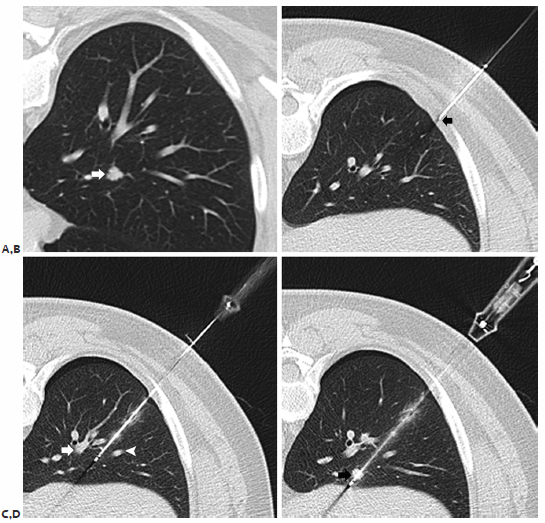
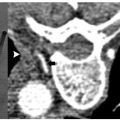
An understanding of the central bronchovascular computed tomography (CT) anatomy provides a safe transthoracic route to a central lesion. The pulmonary hila are composed of the major bronchi with accompanying pulmonary arteries and pulmonary veins that extend radially into the lobes, segments, and subsegments of the lungs. It is often difficult to avoid the vessels and airways in the periphery of the lung, but fortunately, such disturbances result in minimal to no significant complications. For central lesions, when developing a percutaneous transthoracic route, the radial nature of the bronchovascular structures from the hila to the periphery of the lung typically provides an abronchovascular route to the central portions of the lung and thus allowing safe access to a centrally located lesion ( Fig. 6.4 ). By exploiting this abronchovascular plane, the risk of a threatening pulmonary hemorrhage with or without hemoptysis, bronchovascular, bronchopleural fistulas, and, in a worst-case scenario, air embolism can be significantly reduced. In addition to conventional axial images, sagittal and coronal reformations can better delineate the relationship of the target lesion with the surrounding bronchovascular structures and may be beneficial in developing a safe transthoracic route. Of particular interest is the right upper lobe vein tributary (posterior vein) lying in the angle between the anterior and posterior segmental branches, which is present in almost all patients. The clinician should note the possibility of an anomalous pulmonary vein branch seen posterior to the bronchus, which requires special attention so as to avoid injuring it.
As in percutaneous CT-guided lung biopsy, awareness of the interlobar and accessory fissures is important, as these fissures should be avoided to reduce the risk of a pneumothorax, which may result in a problematic or persistent air leak. The fissures are composed of the major, minor, and accessory fissures. The fissures are best visualized on thin, less than 3 mm, CT sections; they appear as a white line that typically can be avoided when developing a path to the target lesion. However, if thin sections are not available, fissural position can be inferred from the location of a 1- to 2-cm-thick avascular plane of lung. The minor fissure is usually difficult to visualize, as it parallels the plane of the scan, but it can be readily visualized on coronal and sagittal reconstructions. The fissures are not always complete, and are often partial. Aziz et al39 catalogued in a large study population the incidence of partial or absent fissures, and found centrally absent right major, left major, and right minor fissures in 48%, 43% and 63% of patients, respectively. Once recognized, incomplete fissure anatomic variation can be taken advantage of while planning a translobar approach to a central lung target ( Fig. 6.5 ). Accessory fissures, seen in up to 30% of individuals,40 should also be considered while planning an approach; common accessory fissures include the inferior accessory fissure that separates the medial basal segment from the remaining basal segments, the azygos fissure (composed of four layers of pleura: two visceral and two parietal) that represents an invagination of the right apical pleura by the azygos vein, the superior accessory fissure that separates the superior segment from the basal segments of the lower lobe, and the left minor fissure that separates the lingula from the remaining portions of the upper lobe.
Lesions adjacent to or within the mediastinum must be approached and ablated with caution, as they pose a risk of injury to mediastinal structures and incomplete ablation from the heat-sink effect. Structures that should be noted when planning a percutaneous thermal ablation include the trachea, aorta, great vessels, superior and inferior vena cavae, heart and pericardium, and esophagus. In addition, depending on the approach and location of the lesion, note should be made of possible injury to neural structures such as the brachial plexus (apical), the left recurrent laryngeal nerve (mediastinal), and the phrenic nerves (juxtamediastinal). Patients and clinicians must be made aware of the potential for injury and the possibility of long-term sequelae following ablation.
Pearls: Anatomic Considerations
Proper placement of coaxial needle is essential for achieving pleural anesthesia and optimal trajectory including tandem placement of the ablation needle.
Abronchovascular route and incomplete fissures provide safe access to central pulmonary lesions.
Ablation near mediastinal structures must be approached and performed cautiously, with great care taken around neural structures.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


