6 Vascular Malformations and Other Vascular Lesions
10.1055/b-0036-141870
6 Vascular Malformations and Other Vascular Lesions
Arteriovenous Malformation
An arteriovenous malformation (AVM) consists of a nidus (tangle) of tightly packed dilated, tortuous arteries and veins, without an intervening capillary network, with the result being arteriovenous shunting. It is the most common symptomatic vascular malformation of brain. The risk of hemorrhage is 2 to 4% per year, with each episode having a 30% risk of death. Most lesions present clinically between 20 and 40 years of age and involve peripheral branches of the ACA or MCA. Aneurysms of the feeding arteries (perinidal aneurysms), due to high flow, are seen in less than 10% of cases. AVMs are considered to be congenital in origin; they are one-tenth as common as aneurysms. Hemodynamically, AVMs have high flow and low resistance.
The nidus of an AVM may be compact or somewhat diffuse. They are often pyramidal in shape, with their base along a cortical surface and their apex directed toward a ventricle (Fig. 6.1). Although not common, there may be hemosiderin staining in the adjacent brain parenchyma due to previous hemorrhage. A total of 65% involve the cerebral hemispheres, 15% the deep midline structures, and 20% the posterior fossa. Most are sporadic in occurrence. Intracranial AVMs occur in about 10% of cases of hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome).
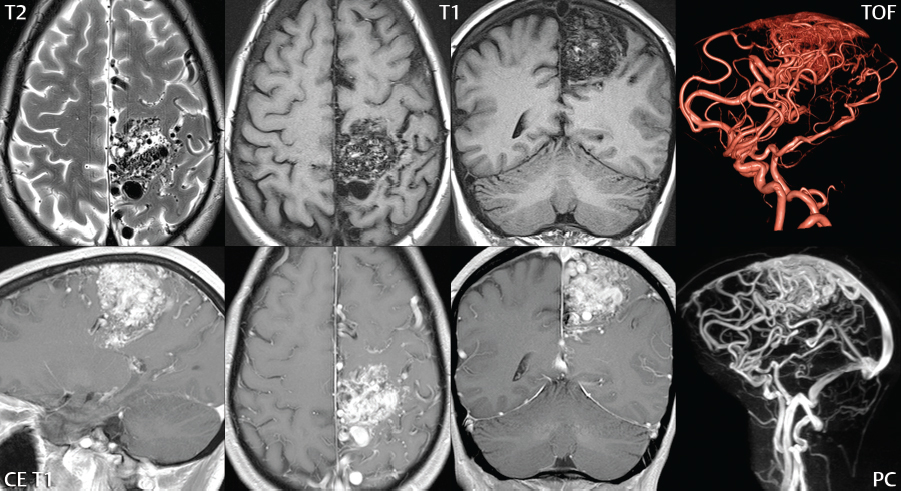
Fig. 6.1 Left paracentral lobule arteriovenous malformation. Flow voids are noted in the left paracentral lobule, together with the precentral, postcentral, and cingulate gyri. There is mild mass effect upon the adjacent brain, best demonstrated on the coronal scans. In regard to MR technique (with the scan performed at 3 T), the precontrast T1weighted scans are obtained with fast spin echo technique and the postcontrast scans with gradient echo technique. The former allows best visualization of the flow voids, and the latter the best visualization of contrast enhancement in both the feeding arteries and draining veins. TOF MRA will visualize predominately the large feeding arteries, together with partial visualization of the nidus and draining veins. The arterial supply is in this instance primarily from the ACA and MCA, with the venous drainage in part via the superior sagittal sinus. Phase contrast MRA can be used, as illustrated, to achieve improved visualization of the venous drainage. The location of the lesion leaves little to no options regarding possible treatment. The paracentral lobule, a continuation of the pre- and postcentral gyri, is supplied by the ACA and controls both motor and sensory innervation for the contralateral lower extremity.
AVMs are well depicted on conventional, crosssectional MR imaging (due to flow phenomena), with TOF MRA used to better demonstrate the nidus, enlarged arterial feeding vessels, and enlarged draining veins. On occasion, a small AVM will be visualized only on MR angiography and not well seen on other MR sequences. On precontrast conventional MR scans, multiple serpiginous vessels, most with low SI due to rapid flow, are typically visualized. Contrast enhancement often provides improved visualization of the nidus, together with the enlarged draining veins (Fig. 6.2; Fig. 6.3).
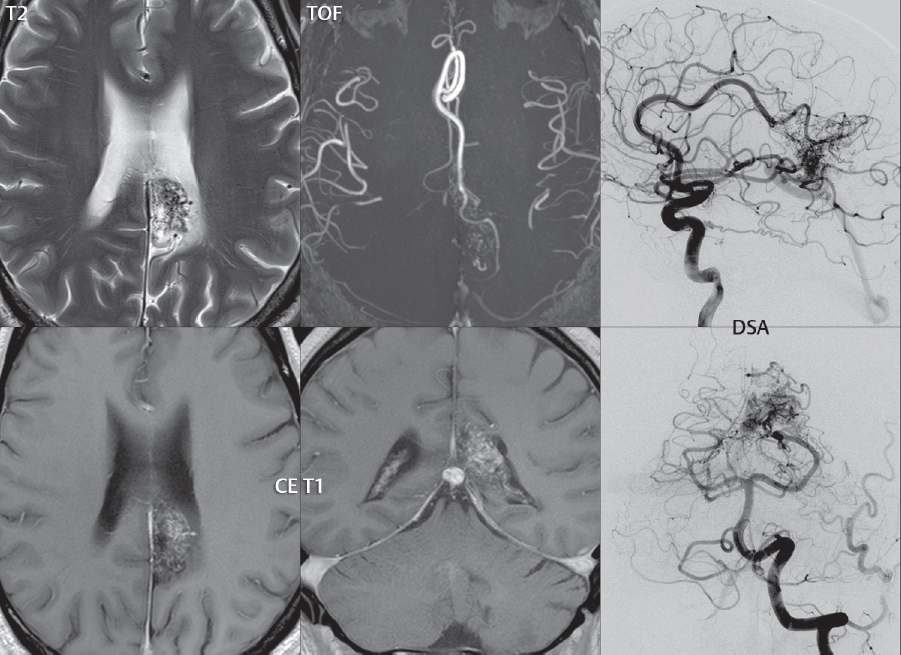
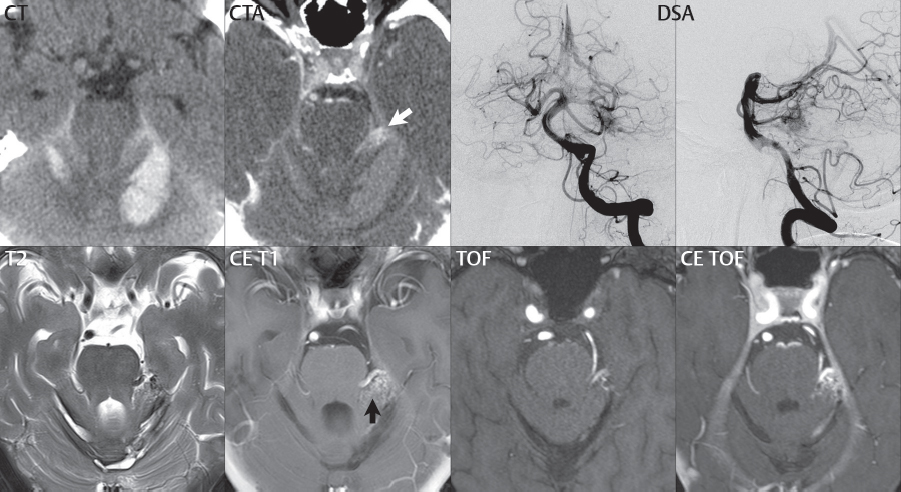
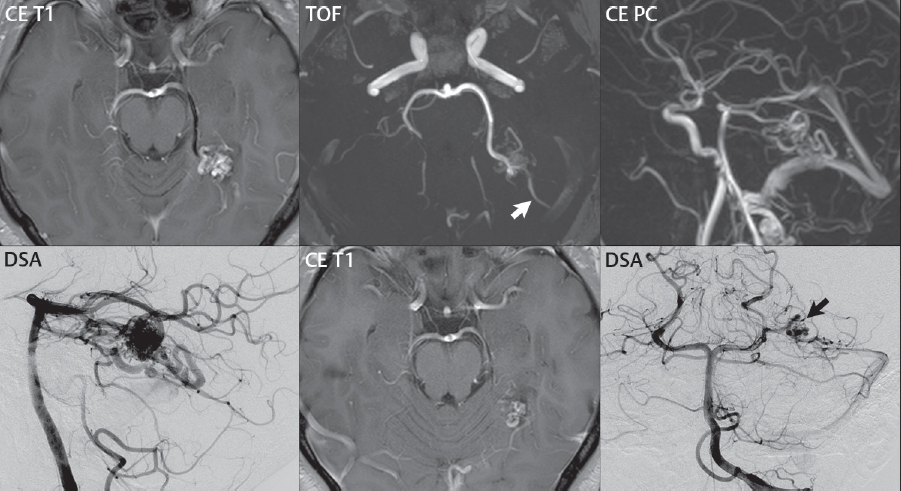
Fig. 6.2 An AVM in the region of the splenium of the corpus callosum on the left, depicted by both MR and DSA. A nidus of small flow voids is noted on the T2weighted FSE axial scan, with corresponding contrast enhancement on the short TE GRE T1weighted axial and coronal scans. A thick MIP axial slab from the TOF MRA reveals the arterial supply from the left pericallosal artery (which is increased in diameter). Although not shown, the left PCA was similarly demonstrated by TOF MRA to supply this AVM. DSA confirms, on lateral and frontal views from left internal carotid and vertebral artery injections, the predominant arterial supply from the distal pericallosal artery and branches of the posterior cerebral artery on the left. Although often not obvious on MR (without prior scans), this AVM had been previously partially embolized.Fig. 6.3 Small left posterior fossa AVM. The patient presented acutely with subarachnoid and intraparenchymal hemorrhage on CT, bilaterally, predominantly confined to the posterior fossa, an unusual pattern for rupture of an intracranial aneurysm. Clinical symptoms included headache, nausea, and dizziness. Although not seen prospectively, close inspection of the CTA reveals an ill-defined enhancing lesion (white arrow), perhaps with a tangle of small vessels, in the left ambient cistern. DSA, with frontal and lateral projections illustrated, was performed the following day, revealing a small AVM predominantly supplied by the left superior cerebellar artery. MR performed a week later reveals substantial resorption of the cerebellar hemorrhages, with residual hemosiderin along the rim of each on the T2weighted image. A small tangle of enhancing vessels is identified postcontrast (black arrow), together with a large posterior mesencephalic draining vein (draining subsequently into the basal vein of Rosenthal). Contrast-enhanced TOF MRA, as illustrated, can provide substantially improved depiction of the involved vasculature, in comparison to standard TOF MRA, for AVMs (and, in some instances, also for aneurysms).
Between the large draining veins, there will be preserved normal brain parenchyma. Gliosis is uncommon. There is usually little mass effect, with vasogenic edema unusual. Acute hemorrhage is well visualized on unenhanced CT; however, on such scans, even large AVMs may not be detected. Calcification is seen in the minority of cases. Enhancement on CT (together with CTA) provides visualization of the nidus and large draining veins (Fig. 6.4). DSA remains the gold standard for evaluation of an AVM, with one major advantage being the clarification of feeding vessels and draining veins (Fig. 6.5). For example, for a convexity lesion, contributions from the ACA and MCA can be distinguished. This can also be done currently by MR, but remains a topic for further research and development.
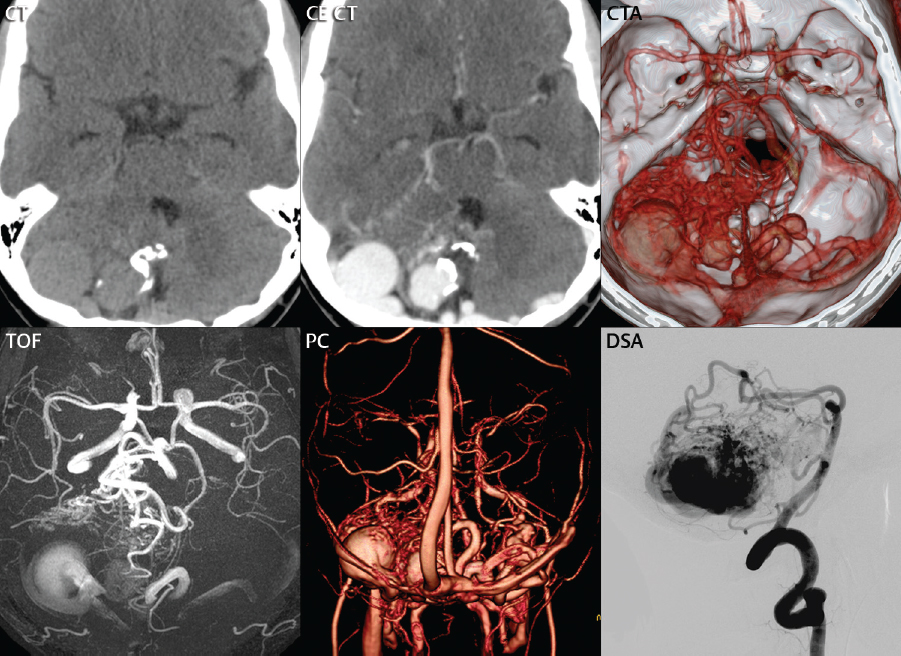
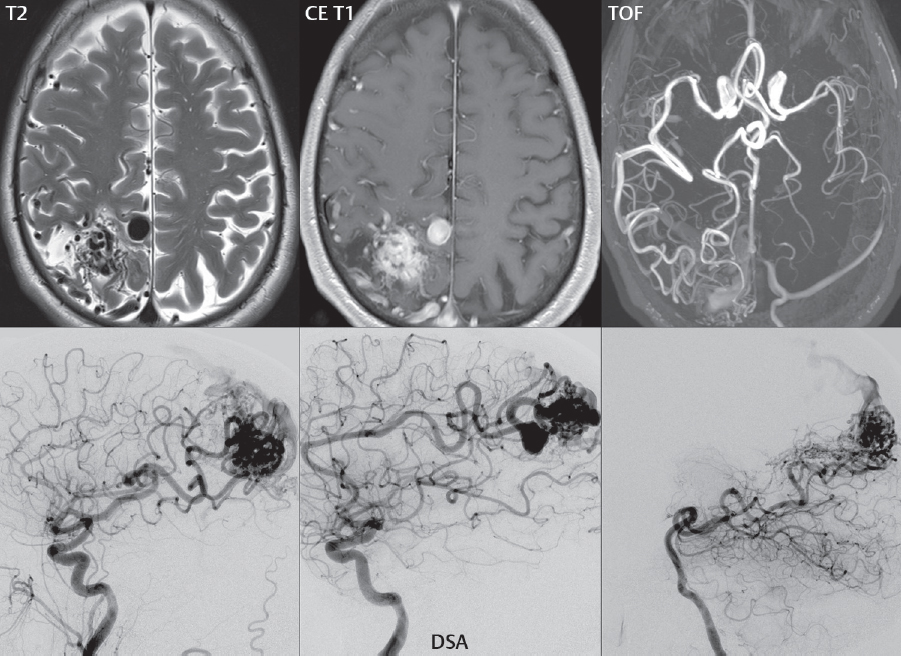
Fig. 6.4 Posterior fossa AVM. Although AVMs can be difficult to detect on unenhanced CT, calcifications, as present with this lesion, are not uncommon and can be a key for diagnosis. There is prominent mass effect upon the adjacent cerebellum, together with mild compression of the fourth ventricle. Both the CTA and the TOF exam demonstrate the arterial inflow to be primarily from the PCA, SCA, AICA, and PICA on the right. The venous outflow is predominately via the right and left transverse sinuses, with a giant venous varix seen on the right.Fig. 6.5 Large right parietal AVM. A tangle of flow voids is noted on the T2weighted scan, lying within the intraparietal sulcus, with the large nidus best identified on the postcontrast T1weighted scan. Although focal atrophy is present, note the absence of associated gliosis, despite the size of this AVM. A large round flow void is identified medially, shown by subsequent imaging (and DSA) to be an aneurysm along a feeding vessel. These are seen in less than 10% of AVMs, are commonly multiple, and are at risk for rupture. The TOF MRA reveals an enlarged right MCA, left ACA, and right PCA, all feeding this AVM. The vascular supply is confirmed by lateral DSA projections obtained from right and left ICA injections, along with an injection of the posterior circulation. The large aneurysm is identified on DSA to involve the distal left ACA.
The risk of hemorrhage from an AVM, from the literature, is 2 to 4% per year. The risk of re-bleeding is increased for several years following a prior hemorrhage. Hemorrhage is the most common presenting symptom (seen in half of all cases) (Fig. 6.6; Fig. 6.7, Parts 1 and 2), followed by seizures (seen in one-quarter).
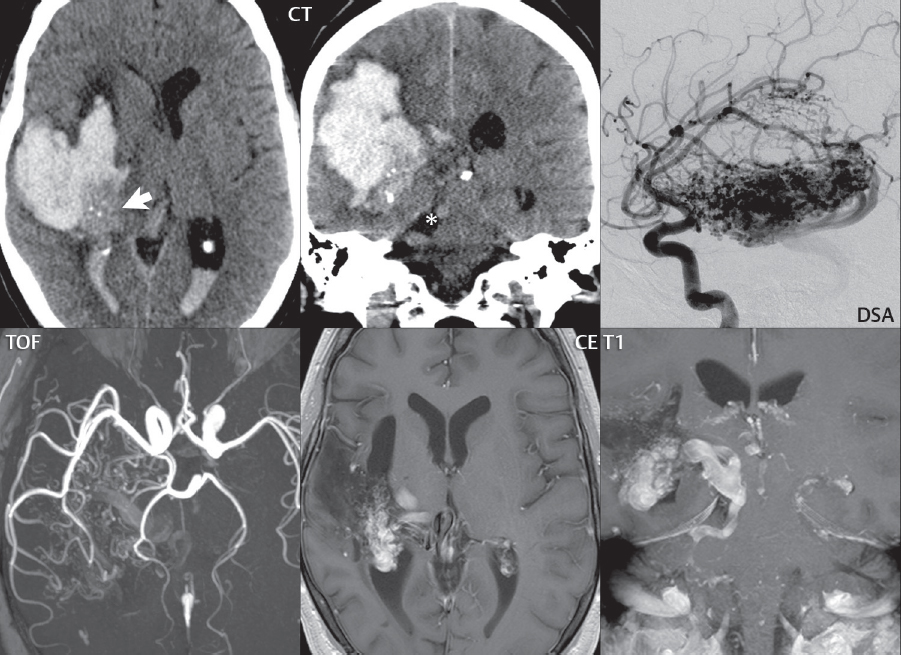
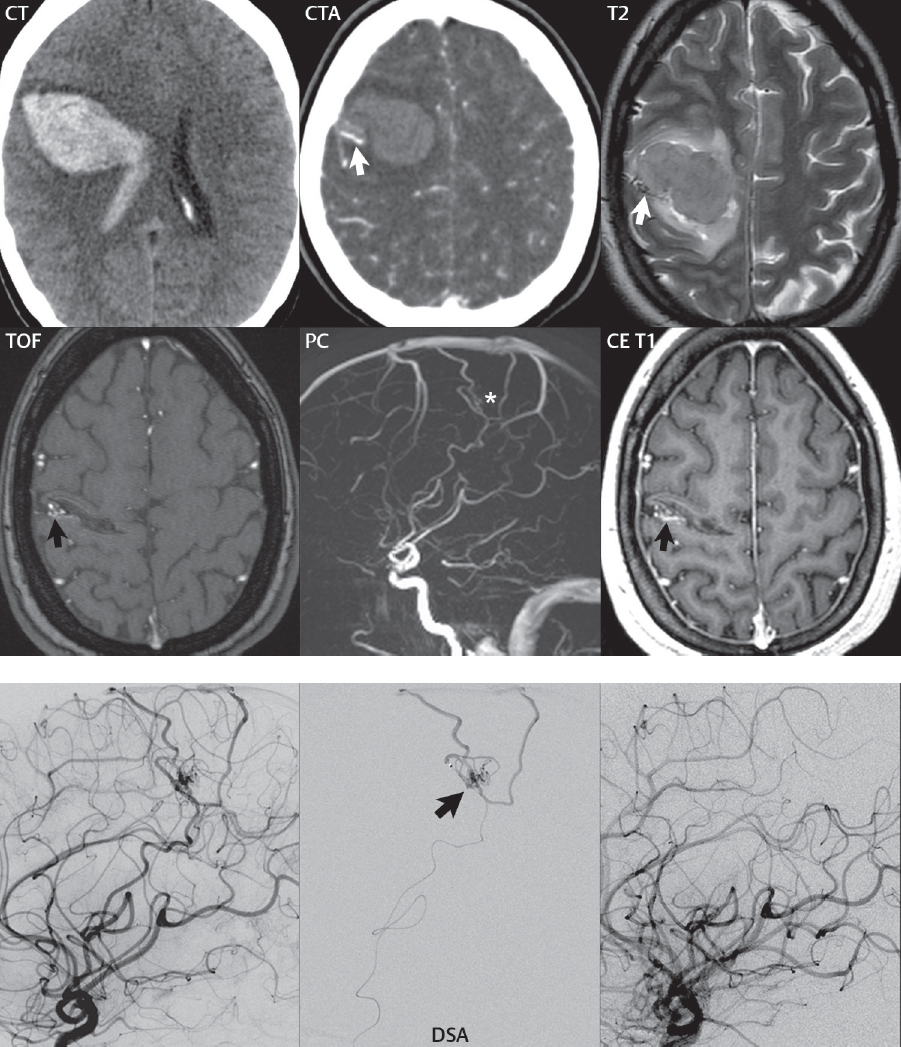
Fig. 6.6 Large retrolenticular AVM, presenting acutely with hemorrhage, but evident due to its size on unenhanced CT performed in the emergency department. On presentation (CT), a large, acute, parenchymal hematoma is noted on the right, traversing the temporal and parietal lobes. There is prominent mass effect, some associated vasogenic edema, and abundant intraventricular blood. Medial, posterior, and inferior to the hemorrhage is an area of intermediate density (white arrow), with punctate calcifications, suggestive of a large AVM. In the perimesencephalic cistern on the right, a large serpiginous draining vein (asterisk) is noted, consistent with this diagnosis. DSA performed in the acute setting reveals a large AVM, which was supplied by the anterior and posterior choroidal as well as the lenticulostriate arteries. Venous drainage was in part by a dilated basal vein of Rosenthal as well as a tortuous, dilated perimesencephalic vein on the right, the latter draining into the superior petrosal sinus. The latter corresponds to the large vein identified on CT. The bottom row of images, from MR, was acquired 1 year later. A thick MIP axial slab from the TOF MRA again demonstrates feeders from both the anterior and posterior circulation on the right. The nidus and a part of the venous drainage are seen on the postcontrast axial T1weighted scan (performed with a short TE GRE T1weighted technique at 3 T, which maximizes visualization of both large and small arteries and veins). Note also the extensive cystic encephalomalacia (with low SI), residual from the prior hemorrhage. A thin MIP of the 2D coronal contrastenhanced T1weighted scan depicts part of the nidus and more effectively displays a portion of the venous drainage medially.Fig. 6.7 Acute parenchymal hemorrhage, with a small underlying AVM noted on followup MR obtained 6 months following presentation (with the interval time allowing for resolution of mass effect and near complete resorption of the hematoma). At presentation on CT, and 6 days later on MR, a large frontoparietal parenchymal hematoma (with extravasation into the lateral ventricle) is noted with mild surrounding vasogenic edema (Part 1). Although not noted prospectively, in retrospect on the CTA, there is the question of an abnormal vein (white arrow) immediately posterior and lateral to the hematoma and, on the MR, both a small tangle of flow voids and the associated slightly prominent vein (white arrow). A common recommendation is to re-evaluate the patient on MR after a sufficient time interval to allow resorption of the hematoma, which was done in this instance. On that followup exam, a small tangle of vessels is noted immediately adjacent and lateral to the small residual fluid cleft on the TOF MRA (black arrow) and on phase contrast MRA (asterisk), which is noted to enhance postcontrast (black arrow), with the latter exam also demonstrating again the slightly enlarged draining vein. DSA (Part 2) was subsequently performed, demonstrating this small plexiform AVM in the precentral sulcus, supplied by a branch of the right MCA. The AVM itself (black arrow) and its drainage into the superior sagittal sinus via two cortical veins are best demonstrated on the superselective injection. Following embolization of the nidus with polyvinyl alcohol, repeat angiography shows complete obliteration of the AVM.
Treatment includes surgery, radiosurgery, and embolization. Asymptomatic lesions, difficult to treat lesions, and patients at high risk for complications warrant conservative treatment. Lesions are stratified according to surgical risk by the Spetzler-Martin grading system, which assigns points relative to size, location, and venous drainage. Lower grade lesions have lower permanent morbidity and mortality following surgery (for example, with permanent morbidity < 5% and mortality < 4% in Spetzler-Martin grades I-III). Surgery can be delayed following hemorrhage, given that AVMs do not have the high, immediate risk of rehemorrhage that aneurysms do. Either intraoperative or postoperative DSA should always be performed to confirm complete obliteration of the lesion. Although uncommon, cerebral edema can occur after surgery and can also be seen with embolization. Surgery may carry a higher cure rate and a lower rehemorrhage risk when compared to radiosurgery.
Radiosurgery delivers a high radiation dose to the isocenter, with a substantially lower dose to nontargeted structures. Current treatment systems include the Gamma Knife and linear accelerator platforms (e.g., the X-Knife and the CyberKnife). Radiotherapy causes endothelial damage, leading eventually to stenosis of the vessels in the treated area and subsequent occlusion. This approach is minimally invasive, low risk (but specifically not free of complications, with permanent neurologic deficits seen in 5%), and effective for smaller lesions (≤ 3 cm). Its disadvantage is that obliteration is delayed, occurring over 2 to 3 years following treatment.
Embolization can be performed for palliation (treatment of part of the lesion) or prior to surgery (Fig. 6.8, Parts 1 and 2). The latter is performed to reduce the volume of the nidus and to occlude feeders that might be difficult to reach by surgery. Cure rates (complete obliteration) are low for treatment of AVMs with embolization alone (5–10%) (Fig. 6.9). This is likely due to the fact that few AVMs have a single pedicle, or just a few pedicles, that can be safely embolized. Embolization materials include polyvinyl alcohol, N-butyl2-cyanoacrylate, and Onyx.
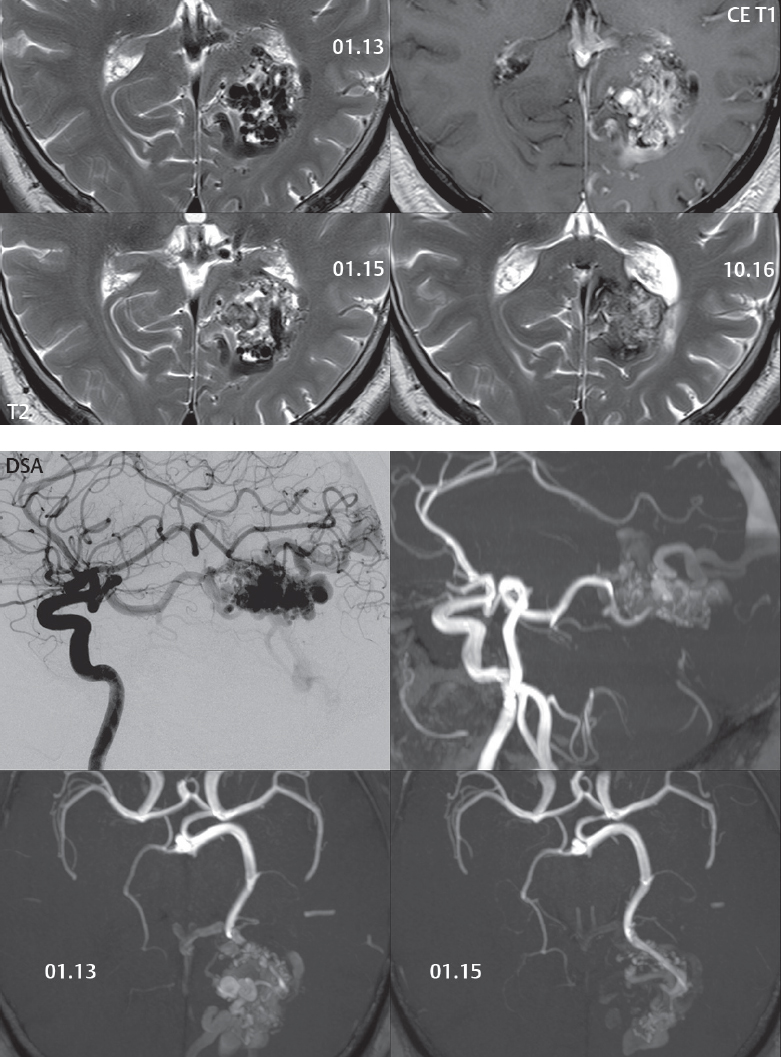
Fig. 6.8 Embolization of an occipital arteriovenous malformation. On the 01.13 MR exam (Part 1), prior to treatment, a tangle of flow voids representing both the nidus and enlarged draining veins is noted medially in the left occipital region, with enhancement postcontrast of the majority of the lesion. On 01.14, several pial branches of the posterior cerebral artery were embolized with cyanoacrylate. On the 01.15 followup MR, there is a reduction in flow voids, along with a reduction in caliber of the draining veins above the nidus (not shown). One year and 9 months later, on the 10.16 MR, there is further thrombosis with near complete obliteration of the AVM (note the absence of flow voids). Prior to treatment, a lateral projection from the DSA and a sagittal MIP from the TOF exam (Part 2) depict well this large occipital AVM, with supply by the PCA (as well as from the anterior circulation via a large PCOM) and drainage into the superior sagittal sinus. Note the reduction in the nidus and as well as the large draining veins in comparing the axial thick MIPs from the TOF MRAs prior to (01.13) and following (01.15) the partial embolization.Fig. 6.9 Left posterior parahippocampal AVM. On the postcontrast axial T1weighted scan, the nidus of this AVM is well visualized, together with its primary arterial supply from the left posterior cerebral artery (seen as a flow void due to fast flow). A small amount of hemosiderin is present, with low signal intensity on this 2D gradient echo scan, adjacent to the nidus, consistent with prior hemorrhage. The thick MIP TOF axial section illustrates both the arterial supply as well as the drainage via a superficial cortical vein (white arrow) into the left transverse sinus. The contrastenhanced PC thick MIP sagittal projection depicts well both the nidus and the enlarged draining veins, as seen in comparison to the lateral DSA projection. Following embolization, there was complete obliteration of the lesion (image not shown). On the followup axial postcontrast MR obtained at 1 year, a small nidus of enhancement is visualized, consistent with partial recanalization. This recurrence (black arrow) is confirmed on the frontal projection from the subsequent DSA, with the lesion then embolized for a second time.
Associated aneurysms are found in less than 10% of AVMs. These may involve feeding arteries (perinidal) (Fig. 6.5) or be intranidal, with the latter distinguished from venous varices on DSA by their visualization in the arterial phase. The risk of hemorrhage from an AVM is increased by the presence of an associated aneurysm.
Large (Spetzler-Martin grade IV-V), as well as giant (> 6 cm), AVMs are difficult to treat. Morbidity and mortality with surgery are high. Partial treatment appears not to reduce the risk of hemorrhage; thus, any treatment should be aimed at eventual complete obliteration.
Cerebral proliferative angiopathy (diffuse cerebral angiomatosis) is a rare vascular malformation with several distinguishing characteristics from a classic AVM. These include large size (lobar or hemispheric), absence of dominant feeders and large (and/or early) draining veins, additional meningeal artery involvement, and normal brain intermingled between vessels.
Only gold members can continue reading. Log In or Register to continue