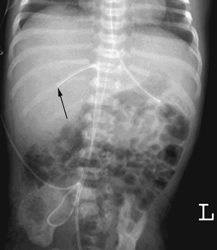
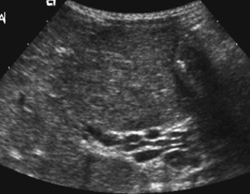
CASE 66 A neonate born to a diabetic mother presents with hypoglycemia and hypertension. Figure 66A Figure 66B (See Color Plate 66B.) Ultrasonography shows an echogenic thrombus within the left portal vein (Fig. 66A), which is occluded. Patency of the left hepatic artery (Fig. 66B) is noted. The left hepatic artery flow was prominent compared with the right hepatic artery. Figure 66C Abdominal radiograph of a newborn showing the tip of the umbilical vein catheter projecting in the region of the right portal vein (arrow). Figure 66D Axial image at the level of the porta hepatis demonstrates multiple anechoic areas of vascular origin on ultrasound representing cavernous transformation of the portal vein. Thrombosis of the left portal vein Portal venous thrombosis is the major cause of extrahepatic portal hypertension and gastrointestinal bleeding in children. Umbilical vein catheterization, commonly used in neonatal intensive care units, is a major cause of portal venous thrombosis (Fig. 66C). Thrombosis may only be detected later in life when established collateral venous circulation, including gastroesophageal varices and cavernous transformation of the portal vein, have already occurred. Portal vein thrombosis is frequently associated with prolonged placement of an umbilical vein catheter. Risk factors include low birth weight, reduced blood flow, hypoxia, and hypercoagulabilitydisorder. Malposition of the catheter in the left portal vein is most problematic, with the umbilicoportal confluence (space of Rex) being the main site of thrombosis. Spontaneous resolution is the usual outcome. Figure 66E CT demonstrating varices along the lesser curvature of the stomach in a child with splenomegaly.
Clinical Presentation
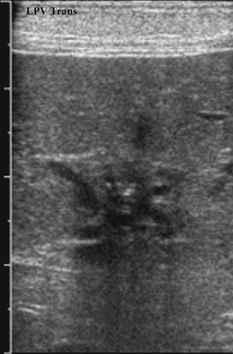
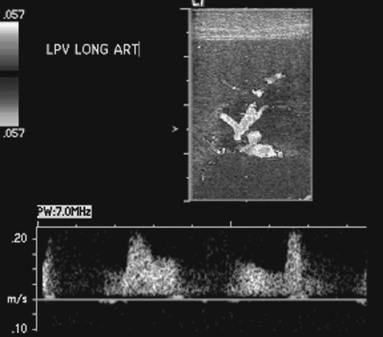
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


