7 Empty Sella Configuration
7.1 Case Presentation
7.1.1 History and Physical Examination
A 70-year-old man with past medical history of hypertension complains of an episode of weakness and tingling in the left upper extremity. MRI was performed to rule out stroke.
The neurological examination was normal.
7.1.2 Imaging Findings and Impression
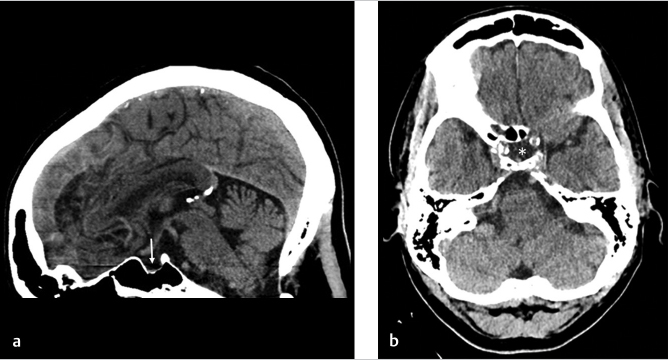
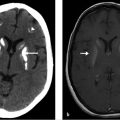
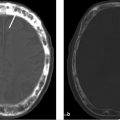
Sagittal (white arrow on ▶ Fig. 7.1a) and axial (asterisk on ▶ Fig. 7.1b) CT scans of the head without contrast show an empty sella configuration filled with cerebrospinal fluid (CSF) and no visualization of the pituitary gland.
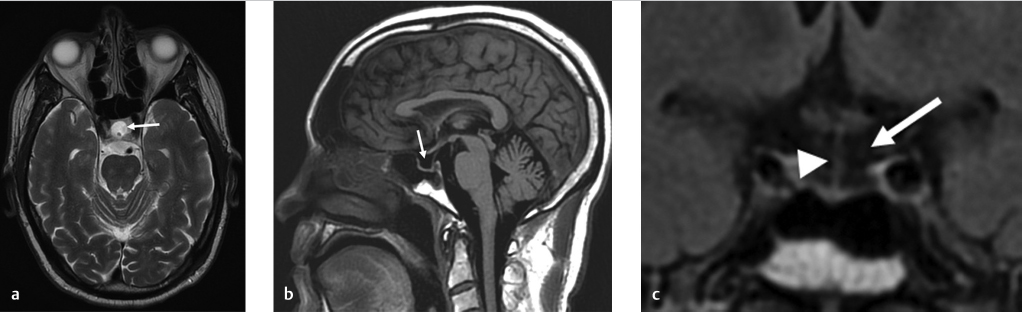
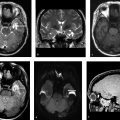
Brain MR images without contrast including axial T2-weighted (▶ Fig. 7.2a), sagittal T1-weighted (▶ Fig. 7.2b), and coronal fluid-attenuated inversion recovery (FLAIR; ▶ Fig. 7.2c) sequences demonstrate an empty sella (white arrows) filled with CSF with nonvisualization of the pituitary gland. However, the pituitary stalk can be visualized (arrow head).
7.2 Differential Diagnosis
Empty sella configuration:
It is seen due to partial or complete absence of the pituitary gland in the sella turcica.
It is a normal-appearing sella filled with CSF with the infundibular stalk traversing it and absence of mass effect or remodeling of sella.
Rathke’s cleft cyst:
It often does not follow the CSF signal intensity on MR images as 50% are of high signal on T1-weighted images.
A small hypointense intracystic nodule may be seen on T2-weighted images and is considered virtually pathognomonic of a Rathke cleft cyst. Small T2 hypointense intracystic nodules may also be present.
Cystic pituitary macroadenoma:
It usually has solid components and septation and does not follow the CSF signal intensity on MR images.
Arachnoid cyst:
Although the signal intensity is very similar to an empty sella, mass effect on the infundibulum will be seen.
In addition, the margins of the cyst may be visible on high-resolution MR images.
Epidermoid cyst:
This tumor is more commonly located in the CP (cerebellopontine) angle, but it can exist in the suprasellar region and can appear very similar to a cyst on T1- and T2-weighted sequences.
It frequently engulfs the adjacent vasculature rather than displacing vessels.
Most importantly, epidermoid cysts are bright on diffusion-weighted images with corresponding dark signal on ADC (apparent diffusion coefficient) due to the presence of keratin.
Incomplete suppression (“dirty CSF”) is seen on FLAIR images.
Craniopharyngioma:
This suprasellar tumor most commonly presents as a multi-loculated cystic and solid mass that frequently calcifies and does not follow the CSF signal intensity.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


