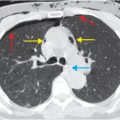
Diagnosis: Right sternoclavicular joint dislocation
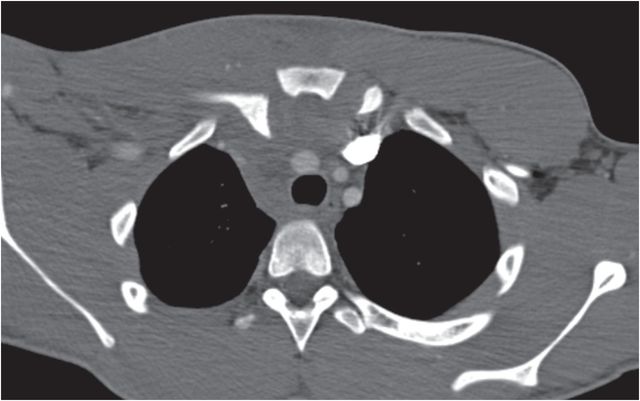
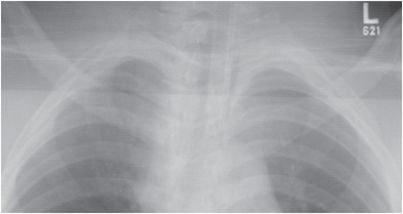
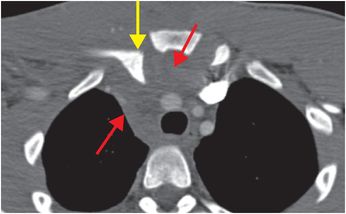
Chest radiograph demonstrates subtle asymmetry in the position of the medial clavicles in this intubated patient. Axial contrast-enhanced CT through the upper chest reveals right posterior sternoclavicular dislocation (yellow arrow) with an anterior mediastinal hematoma (red arrows). The left sternoclavicular joint is normal.
Discussion
Overview of sternoclavicular dislocation
Sternoclavicular dislocation is most often due to high-energy injuries, and can be seen as a result of direct and indirect forces about the joint. Indirect mechanisms are more common, caused by lateral compression of the shoulder girdle.
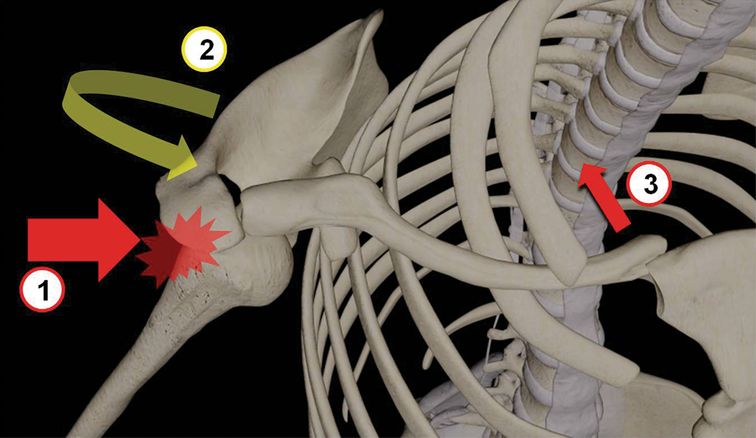
Compressive force on the lateral aspect of the shoulder (1) results in protraction of the scapula (2), with compressive force transmitted along the shaft of the clavicle to produce posterior dislocation at the sternoclavicular joint (3). Alternately, if the compressive force vector causes retraction (rather than protraction) of the scapula, then anterior dislocation of the clavicle at the sternoclavicular joint can result.
The classification of sternoclavicular dislocation primarily depends on the direction of dislocation at the sternoclavicular joint, with anterior dislocations occurring much more commonly.
Posterior dislocations have an increased risk of associated soft tissue injuries, including injuries to the great vessels or the trachea.
Patients under 25 years old may have injury to the proximal clavicle physis.
Imaging of sternoclavicular dislocation
Sternoclavicular dislocations are usually occult or very difficult to see on standard chest radiographs. Sometimes slight asymmetry in the alignment of the sternoclavicular joints can be seen, although this finding can be difficult to distinguish from positional variation.
Serendipity views (frontal radiograph with 40 degree cephalic tilt) can better show the anterior and posterior displacement.
CT is recommended for full characterization of extent of injuries, particularly vascular, tracheal, or lung injuries in the setting of posterior dislocations. Dyspnea or dysphagia can result from compression of the trachea and esophagus in posterior dislocations.
Treatment issues
Early closed reduction can be attempted, though surgical reduction is often required.
Posterior dislocations should undergo urgent reduction in an operative setting due to the high risk of associated soft tissue injuries.
Over-reduction of anterior dislocation can cause injury to underlying chest structures, including the great vessels, trachea, and lungs. Closed reduction of anterior dislocations should therefore be performed only with close coordination with thoracic surgery.
Related posts:
 12 68-year-old man with left lower quadrant pain and hypotension
12 68-year-old man with left lower quadrant pain and hypotension
 32 32-year-old male complaining of chest pain after upper endoscopy
32 32-year-old male complaining of chest pain after upper endoscopy
 28 30-year-old male presented with a palpable left testicular mass
28 30-year-old male presented with a palpable left testicular mass
 29 19-year-old male presented with acute onset right scrotal pain
29 19-year-old male presented with acute onset right scrotal pain
 53 42-year-old female presenting with fever and back pain
53 42-year-old female presenting with fever and back pain
 66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
66 21-year-old male with quadriplegia after diving into a shallow pond. The patient struck his head against an embankment, with his head flexed, chin against chest
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


