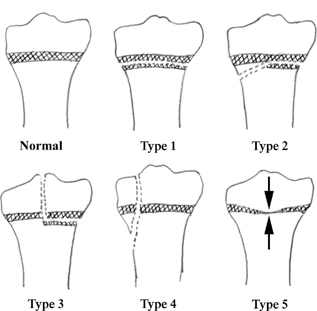
CASE 93 A 14-year-old male with a previous history of Salter-Harris type 2 fracture of the distal femur presents with leg-length discrepancy (LLD). Figure 93A Figure 93B Frontal radiograph of distal femur demonstrates loss of lucent physeal plate visualization centrally (Fig. 93A). Coronal spoiled gradient echo (SPGR) MRI demonstrates loss of normal high-signal intensity physeal plate visualization centrally with spanning bridge of isointense signal between metaph-ysis and epiphysis (Fig. 93B). Figure 93C Illustration of five types of Salter-Harris injury with damage to physeal plate depicted. Traumatic bone bridge formation with growth plate arrest Physeal plate injury in children is common, and when associated with bony bridge formation and/or subsequent growth arrest can result in lifelong disability. The vast majority of cases are post-traumatic with an estimated incidence of physeal fracture of 3 in 1000. Seventy-five percent of these injuries occur between the ages of 10 and 16 years. The Salter-Harris classification of physeal plate fractures described more than 40 years ago is still widely used today, with higher grades showing increasing likelihood of growth plate injury (Fig. 93C). The risk of physeal plate dysfunction depends on the fracture type, underlying growth potential, anatomic site, and severity of injury. Significant displacement, comminution, or loss of a segment of germinal or proliferative layer of physeal cartilage increases the risk of future growth arrest. Independent of cause, growth plate arrest and bone bar/bridge formation are more common in the lower extremities. Posttraumatic bone bars usually involve the distal physeal plates, whereas bridges from other causes are more common at proximal physeal centers. Although the distal radius and phalanges are the most common sites for physeal plate fractures, the distal femur and tibial physeal plates are more likely (16 to 35%) to undergo growth arrest post-trauma. Physeal plate arrest is most often the result of previous trauma. Fifteen percent of all pediatric fractures involve a physis, and ~15% of these fractures will subsequently suffer growth plate dysfunction. Infection, tumor, irradiation, burns, frostbite, electrical trauma, vitamin A toxicity, surgical procedures and underlying sensory neuropathy, sickle-cell disease, and metabolic abnormalities have all been documented to occasionally result in growth plate disturbance. Some patients with poliomyelitis and multiple dysplasias, including osteopetrosis, are associated with physeal dysfunction and secondary metaphyseal dysfunction. Figure 93D Frontal radiograph of distal femur depicts loss of visualization of physeal plate centrally (arrowheads) with bone continuity across physis from metaphysis to epiphysis at this site. Figure 93E
Clinical Presentation


Radiologic Findings
Diagnosis
Discussion
Background
Etiology


![]()
Stay updated, free articles. Join our Telegram channel







Full access? Get Clinical Tree


