 Clinical Presentation
Clinical Presentation
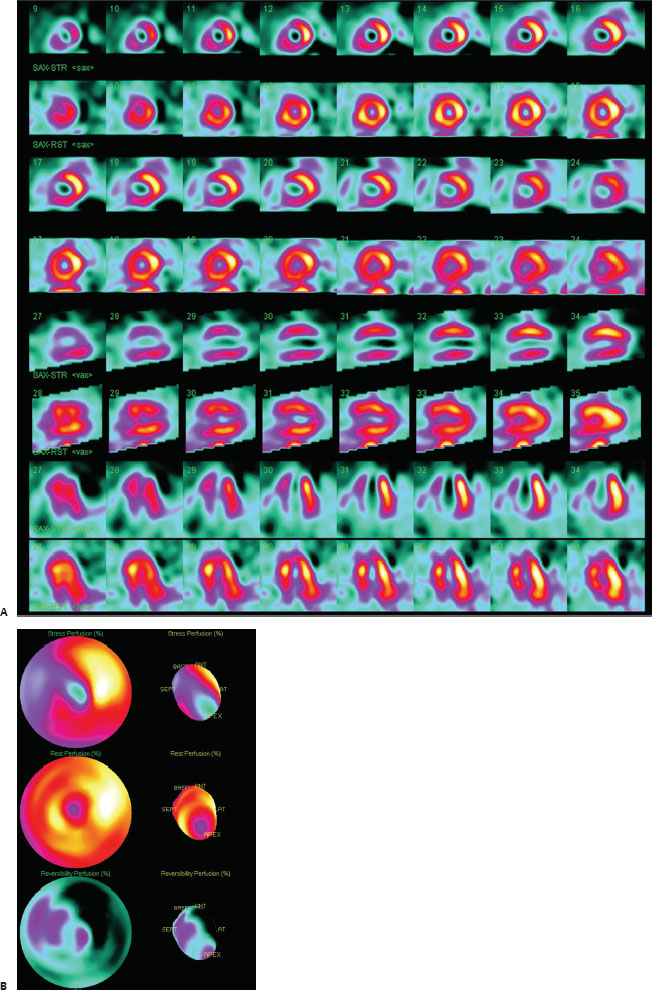
A 64-year-old woman with chest pain on exertion.

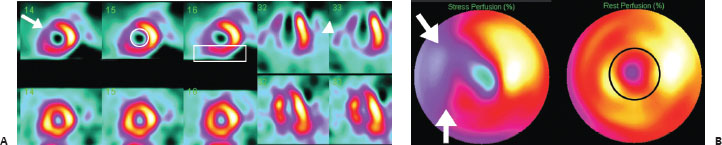
(A) Rest and stress myocardial perfusion scintigraphy demonstrates a large, severe, almost completely reversible perfusion defect in the anteroseptal and apical segments (left anterior descending territory; arrow) with a moderate, completely reversible defect in the inferior wall (right coronary territory; rectangle). Additionally, increased right ventricular (RV) uptake (arrowhead) and an increase in left ventricular (LV) chamber size (“transient ischemic dilation”; circle) are seen at stress. (B) Rest and stress polar maps and surface renderings display the same nearly completely reversible abnormalities (arrows). A small apical perfusion defect persists at rest (circle).
 Differential Diagnosis
Differential Diagnosis
• Reversible ischemia in the left anterior descending (LAD) artery and right coronary artery (RCA) territories: Reversible perfusion defects indicate that this is the most likely diagnosis. (The small fixed apical component may represent a small superimposed infarct.)
• Shifting breast artifact: This can occasionally simulate reversible LAD artery disease. However, it would not affect the inferior wall.
• Diaphragmatic creep artifact: This can simulate reversible RCA disease. However, it would not affect the anterior wall. It is rarely encountered with current imaging protocols.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


