A Radiographic Anthology of Vertebral Names*
Terry R. Yochum
Bryan Hartley
David P. Thomas
Gary M. Guebert
The material in this chapter formed the basis for the first scientific exhibit ever accepted for display at the Radiological Society of North America (RSNA) by a chiropractor or from the country of Australia. The exhibit was displayed in Chicago in November 1982 and was titled “By Their Names You Will Know Them.” The exhibit was honored by receiving an RSNA Honorable Mention Citation.
INTRODUCTION
“Since biblical times in the Tower of Babel men have ceased to speak a universal language. This is particularly true in the healing arts where the use of medical jargon frequently prevents physicians from communicating accurately.” (1)
Before the turn of the twentieth century many radiologists appreciated this difficulty and used their imagination to overcome it. The literature has thus become replete with descriptive appearances, for example, “names.” Benjamin Felson stated: “A (sic) name saves time, helps you to remember the sign, and advertises it. A sobriquet selected should be appropriate and on target.” (2) A total of 88 such named vertebrae have been extracted from the literature. With so many names from scattered sources, we thought it helpful to collate them in a single presentation.
A short description is given when appropriate, and the anatomic and pathogenic reasons for the appearances are briefly considered. A list of conditions associated with each named vertebra, when appropriate, accompanies the descriptive paragraph. The named vertebrae are presented in alphabetical order.
Accessory Transverse Process Sign. This term denotes lack of continuity of the transverse process with the lumbar vertebra. This floating transverse process, when associated with absence of the ipsilateral pedicle shadow at the same level, is an additional supportive roentgen sign of a congenital origin.
Pedicle agenesis in the lumbar spine (3)
Bamboo Spine (Poker Spine). This refers to the appearance seen in an anteroposterior (AP) projection of the lumbar spine. The appearance is the result of symmetrical bridging of multiple intervertebral disc spaces by marginal syndesmophytes. (Fig. 17-1)
Ankylosing spondylitis (4)
Psoriatic arthritis (5)
Enteropathic spondylitis (5)
Reiter’s syndrome (6)
Following poliomyelitis (occasionally) (7)
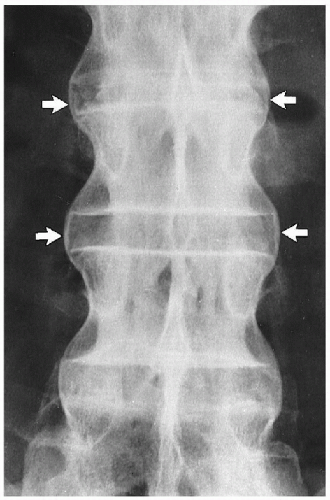 Figure 17-1 BAMBOO SPINE (arrows). Ankylosing spondylitis. |
Barrel-Shaped Vertebra. This vertebra is seen in the lateral projection. Owing to complete resorption of the anterosuperior and inferior body margins and reactive midbody osteitis, the anterior contour assumes a convex contour. (Fig. 17-2)
Ankylosing spondylitis (8)
 Figure 7-2 BARREL-SHAPED VERTEBRA (arrow). Ankylosing spondylitis. (Courtesy of Gerald A. Fitzgerald, MD, Sydney, Australia.) |
Beaked Vertebra (Notched or Hooked Vertebra). This anomaly is seen in the lateral projection. Anterosuperior vertebral body notching leads to kyphosis. (9)
Achondroplasia (9)
Diastrophic dwarfism (9)
Spondyloepiphyseal dysplasia (9)
Trisomy 21 syndrome (Down’s syndrome or mongolism) (9)
Werdnig-Hoffman syndrome (familial spinal muscular atrophy) (9)
Trauma (battered child, non-accidental trauma syndrome) (9)
Mucopolysaccharidosis I (Hurler’s syndrome) (9)
Mucopolysaccharidosis IV (Morquio’s syndrome) (9)
Phenylketonuria (9)
Biconcave Lens Vertebra. This vertebra is seen in the lateral projection. It is the result of softening of the vertebra, which becomes narrow in the center after weight bearing begins. (Fig. 17-3)
Osteogenesis imperfecta (12)
Blind Vertebra. This vertebra is seen in the AP projection and is a direct result of bilateral destruction of the pedicles. (Fig. 17-4)
Osteolytic metastatic carcinoma (13)
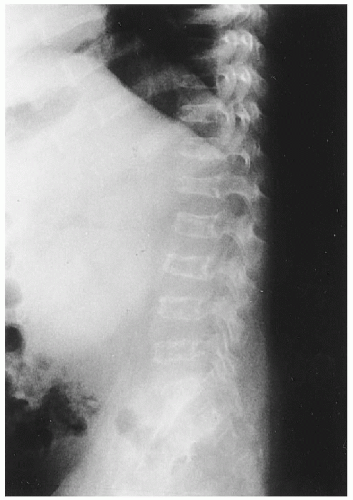 Figure 17-3 BICONCAVE LENS VERTEBRA. Osteogenesis imperfecta. |
 Figure 17-4 BLIND VERTEBRA (arrows). Osteolytic metastatic carcinoma. |
Bone within a Bone. This may be seen in both AP and lateral projections, as well as in the oblique view. (Fig. 17-5)
Normal infants (14)
Cleidocranial dysplasia (12)
Osteopetrosis (12)
Gaucher’s disease (17)
Oxalosis (18)
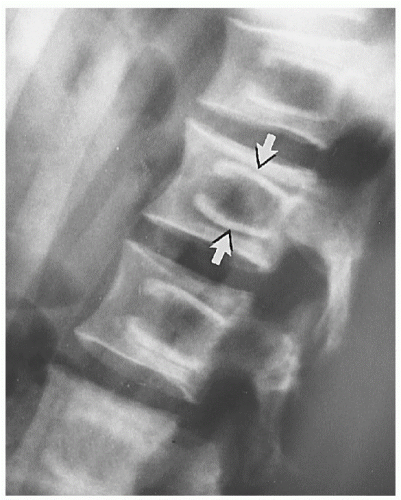 Figure 17-5 BONE WITHIN A BONE (arrows). Osteopetrosis. |
Bottle-Like Vertebra. This is seen in the thoracic spine in the lateral view, on which the posterior portions of the intervertebral disc spaces appear widened compared with the central portion of the body. (Fig. 17-6)
Hypothyroidism (10)
 Figure 17-6 BOTTLE-LIKE VERTEBRA. Hypothyroidism (cretinism). (Reprinted with permission from The Center for Devices in Radiological Health, the FDA, and the American College of Radiology: The Learning File, Skeletal Section, SK-508.) |
Bowline of Brailsford (Gendarme’s Cap, Inverted Napoleon’s Hat). This vertebra is seen in the AP projection of the L5 vertebra, on which the caudally displaced vertebral body represents a curved density below the level of the sacral base. (1) (Fig. 17-7)
Spondylolisthesis (types III and IV)
 |
Bullet-Nosed Vertebra. This is caused by wedging of the anterior aspect of the vertebral body, resulting in a kyphosis. (Fig. 17-8)
Butterfly Appearance. This abnormality is seen in elderly patients in the AP view. It is the result of bone softening, which allows protrusion of disc material into the weakened adjacent vertebral endplates.
Paget’s disease (10)
Butterfly Vertebra. There are two types of butterfly vertebra. (20)
Type I (or double-D) depends on the persistence of a sagittal cleft and is seen in the AP view. (Fig. 17-9) Type II (or doublewedge) depends on the persistence of both sagittal and coronal clefts and is seen in the AP and lateral views.
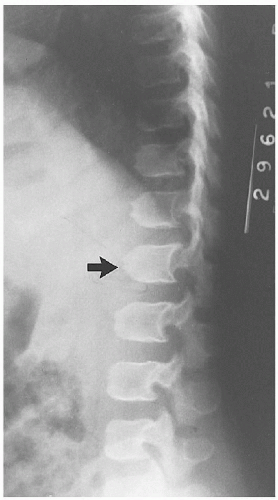 Figure 17-8 BULLET-NOSED VERTEBRA (arrow). Achondroplasia. (Courtesy of Paul E. Siebert, MD, Denver, Colorado.) |
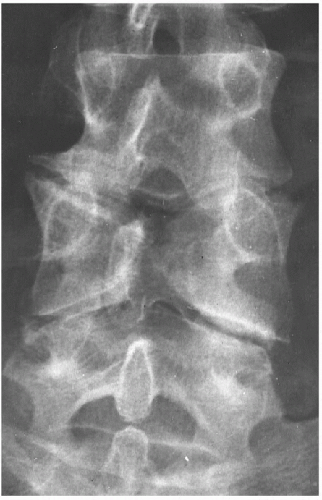 Figure 17-9 BUTTERFLY VERTEBRA. Congenital midline defect. |
Charcot Spine (5). See Jigsaw Vertebra.
Clover Leaf Vertebra. This is seen in the vertebral bodies and is arranged like clover leaves. Globular radiolucencies become surrounded by densities of calcium.
Rickets (less acute stage) (21)
Codfish Vertebra. This is seen in the lateral projection. There is increased concavity with a smooth curvature of the superior and inferior vertebral margins owing to bone softening.
Osteomalacia (22)
Coin-on-End Vertebra (Silver Dollar, Vertebra Plana, Wafer-Thin Vertebra). This appearance is the result of compression of the vertebral body. Uniform density is noted, and it is wider than normal in both sagittal and coronal planes. (Fig. 17-10)
Eosinophilic granuloma (23)
 Figure 17-10 COIN-ON-END VERTEBRA (arrow). Eosinophilic granuloma. |
Corduroy Cloth Vertebra (14) (Honeycomb Appearance [10], Striated Vertebra [13]). This represents an accentuation and thickening of the vertically oriented trabeculae of the vertebral body. (Fig. 17-11)
Corner Vertebra (Step-Off Vertebra). This is the result of an anterolateral defect in the vertebral body and is seen in the lateral view. It may give rise to kyphoscoliosis. (24)
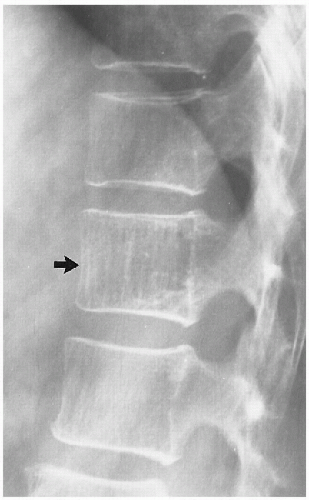 Figure 17-11 CORDUROY CLOTH VERTEBRA (arrow). Intraosseous hemangioma. |
Cupid’s Bow Contour. This vertebra is seen in the AP view of the lower lumbar spine, where the inferior endplates of the L3-L5 bodies frequently have paired parasagittal upward concavities. (Fig. 17-12)
Normal variant (25)
Cupped Vertebra (9) (H Vertebra [15]). This is the result of central depression in the endplate that occurs with an abrupt transition to the more normal periphery. Usually best seen in the lateral view, but may also be seen in the AP view. (Fig. 17-13)
 Figure 17-12 CUPID’S BOW CONTOUR (arrows). Normal variant. |
Dog Spine. This is seen in the lateral view when the AP dimension of the body is reduced and thus there is relative increase in the posterior vertical measurement. The spine assumes a posteriorly curved appearance, simulating that seen in a dog’s spine.
Ependymoma (10)
Double Contour Spine. This anomaly has a similar appearance to a bone within a bone. It is produced by the same process.
Infantile cortical hyperostosis (26)
Double Spinous Process Sign. On the conventional AP view of the cervical spine, one can identify a double shadow of the spinous process owing to caudal displacement of the avulsed fragment. (Fig. 17-14)
Clay shoveler’s avulsion fracture (27)
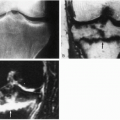
Empty Vertebra. This is seen in the AP view of the spine. Horizontal fractures through both pedicles and transverse processes produce a horizontal lucent defect that is projected over the body of the involved vertebra. (Fig. 17-15)
Chance (lap seat belt) fracture (1)
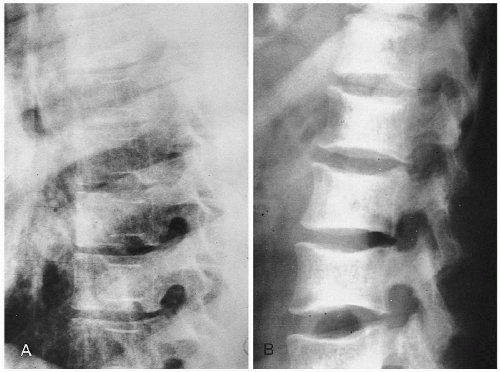 Figure 17-13 THE CUPPED VERTEBRA. A and B. Sickle cell anemia. This is also known as the H vertebra. |
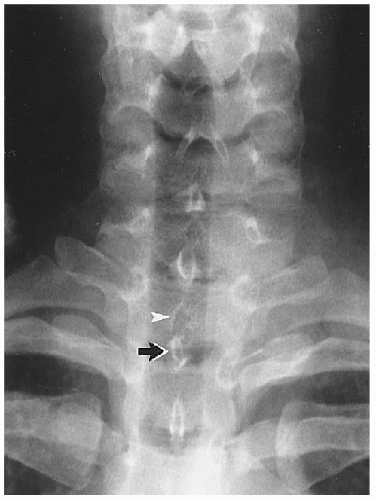 Figure 17-14 DOUBLE SPINOUS PROCESS SIGN. Observe the caudally displaced avulsion of the spinous process of T1 (arrow); the remaining spinous process is seen (arrowhead). |
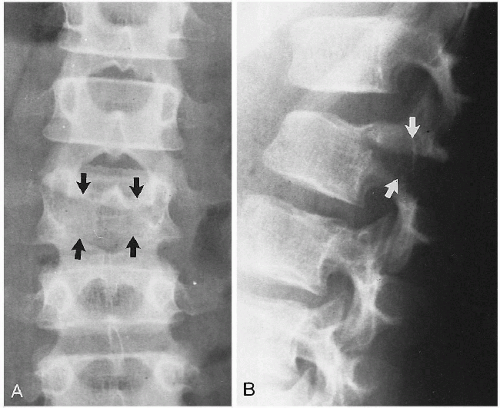 Figure 17-15 EMPTY VERTEBRA (arrows). A and B. Lap seat belt fracture (Chance’s fracture). |
Fish Vertebra (Codfish Vertebra, Fishbone Vertebra, Hourglass Deformity). The shape of the vertebral body conforms to upward and downward bulging of the intervertebral disc. This simulates the vertebral shape found in fish. (Fig. 17-16)
Hyperparathyroidism (primary and secondary) (26)
Neurofibromatosis (26)
Juvenile idiopathic osteoporosis (28)
Rickets (28)
Hand-Schüller-Christian disease (28)
Sickle cell anemia (29)
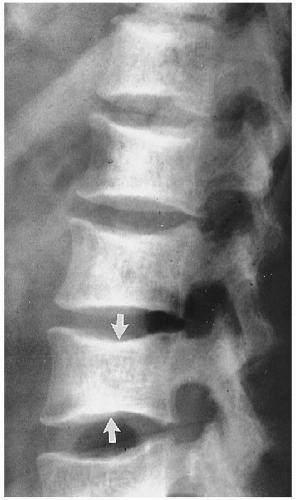 Figure 17-16 FISH VERTEBRAE (arrows). Sickle cell anemia. |
Fishbone Vertebra. See Fish Vertebra.
Flame-Shaped Vertebra. This vertebra is seen on the lateral view of the spine. The superior and inferior vertebral endplates taper to form a central beak. (Fig. 17-17)
Mucopolysaccharidosis IV (Morquio’s syndrome) (28)
Frame-Like Vertebra. This occurs when the vertebral bodies have an osteosclerotic border with a relatively radiolucent center.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


