Chapter 192
Abscess
Epidemiology
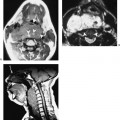
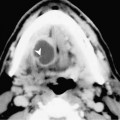
The sublingual space (SLS) is located inferior to intrinsic muscles of the oral tongue, medial to the mandible, and superomedial to the mylohyoid muscle. Posteriorly, the SLS communicates with the submandibular space (SMS) with no fascia separating these spaces. Abscesses originating in this space may be due to sublingual or submandibular duct stenosis or calculus disease. Dental infection or mandibular osteomyelitis may also extend into the SLS.
Clinical Findings
Patients with SLS abscess usually present with pain, tenderness, and swelling in the anterior floor of the mouth. This may be associated with trismus when inflammation involves the medial pterygoid muscle. There may be a history of salivary colic, recent dental disease, or dental manipulation.
Pathology
An enlarging SLS abscess, like a plunging ranula, decompresses posteriorly into the SMS. Because the SMS is more commodious, the submandibular component of the lesion frequently overshadows that of the SLS. As in SMS infection, the most commonly encountered organisms are Staphylococcus aureus and Streptococcus viridans.
Treatment