Figure 21.1 Fatal spinal injury in an abused infant. A, AP postmortem radiograph demonstrates a complex fracture-dislocation at the cervicothoracic junction. B, A pathologic specimen of the spinal column and contents shows complete separation of the spinal column at the cervicothoracic junction. (Courtesy of Nancy Genieser MD.)
History and background
The first radiologically documented case of spinal fractures related to probable child abuse was reported by Astley in 1953 (1). Although he attributed these fractures, as well as other long bone injuries, to an underlying state of metaphyseal fragility, it is apparent that he was describing a group of abused infants. In 1957, Jones and Davis reported an inflicted lumbar spine fracture in one of five abused children (2). Subsequent reports have added to the understanding of inflicted spinal injury (3–37). Articles and texts dealing with child abuse have included examples of spinal lesions (28, 38–66), and general discussions of pediatric spinal trauma have cited cases of inflicted injury (67).
The prevalence of abusive spinal trauma is difficult to determine. In large child abuse series, the percentage of fractures involving the spine based on imaging ranges from 0 to 3% (48, 50, 60, 68–72). In a large study that examined 563 cases of abuse, Merten and colleagues failed to identify a single spinal injury (70). Similarly, in a series of 31 fatally abused infants, Kleinman and colleagues found only one spinal fracture out of a total of 165 skeletal fractures (49).
An early review of the child abuse literature revealed 41 cases of vertebral injury (73). Most of these were vertebral body fractures. Of those fractures involving the posterior elements, most were also accompanied by fractures of the vertebral bodies; only two reports noted isolated posterior element injury (9, 12). The average age at which spinal injuries were recognized was 22 months (range 2 months to 10 years). Over two-thirds of these injuries occurred in children less than three years of age, and half of the children were under one year. A similar age-related incidence for nonspinal fractures was noted. While some children presented with clinical evidence of spinal cord compression or contusion (4, 5, 16, 18), most patients showed no signs or symptoms referable to the spine. Occasionally, an accentuated kyphosis was observed on clinical examination, and sometimes the only apparent indication of severe vertebral subluxation was postural abnormality or stiffness (4, 19).
With the advent of computed tomography (CT) and magnetic resonance imaging (MRI), impressive changes in the imaging patterns of abusive spinal trauma emerged. In 2010, Kemp and associates published a systematic review of the clinical and radiologic characteristics of inflicted spinal injury (74). They performed a literature search of multiple electronic databases, websites, references, and bibliographies from 1950 to 2009. They included studies of inflicted injury involving the vertebrae or spinal contents in children under 18 years of age, alive at presentation, with a high surety of diagnosis of abuse, and sufficient detail to analyze the data. Several early reported cases were excluded from the analysis because of inadequate documentation. The methodologic limitations of the review were well detailed by the authors. In total, they found 19 reports of 25 children that satisfied their study criteria (Table 21.1).
CPR Cardio pulmonary resuscitation, PF=Plain film, RNS radionuclide scan, SAH subarachnoid haemorrhage, SDH Subdural haemorrhage, Skeletal survey SS
In 11 of 25 (44%) cases there was no explanation for the injury, and in 9 cases (36%) minor domestic trauma was reported. In 5 of 25 (20%) cases there was a history of inflicted trauma at presentation and in 7 instances (28%), abuse was subsequently admitted. In 7 children (28%) clinical signs of spinal injury were masked by respiratory symptoms and impaired levels of consciousness, and in 6 of those children, coexistent abusive head trauma (AHT) was present. The diagnosis of abuse was delayed in 14 of 25 cases (56%) and missed in 3 children (12%) who had also been hospitalized previously. Twelve children (48%) (median age: 5 months; range: 1–48 months) had isolated cervical spine injuries, 12 children (48%) had thoracolumbar injuries (median age: 13.5 months; range: 6–16 months), and 1 child (4%) had cervical, thoracic, and sacral injuries. Ten of 12 children with thoracolumbar injuries (83%) had lesions at T11–L2, and 9 of 12 children (75%) had fracture-dislocations. Ten of 12 cases had lumbar kyphosis or thoracolumbar swelling, and only 2 (17%) had focal neurologic deficits. This comprehensive review of abusive spinal injuries is likely weighted to the more severe and complex injuries that are published as case reports. Kemp and associates did not include data published by Levin et al. in 2003 that described the imaging findings in 7 children with thoracolumbar fractures and spondylolisthesis, which were considered abusive injuries (27). Although 2 of the 7 children (29%) were paraplegic on admission, the others had no neurologic signs or symptoms. Recent studies have focused on the incidence of cervical ligamentous injuries in AHT victims. In 2014 Kadom et al. studied 38 children with AHT and found a substantial number with cervical ligamentous injuries, usually in association with intracranial abnormalities (37). Choudhary et al. compared cervical MRIs in 67 AHT victims with examinations in 46 accident victims and found an incidence of cervical ligamentous injury of 78% in the AHT group versus 46% in the accidental group (66) (see below).
Cohort studies assessing the prevalence of spinal injuries detected on skeletal surveys (SSs) indicate that simple vertebral compression fractures of the spine are likely more common than the fracture-dislocations detailed in published cases reports. In a study of 930 SSs performed for suspected abuse in children under 2 years of age, Karmazyn and associates found 3 cases (0.3%) with spinal fractures (60). All fractures were asymptomatic vertebral body compression injuries. Harlan and colleagues reviewed the SSs in 101 children under 3 years of age and found spinal fractures in 3% of children; all were thoracic or lumbar compression injuries (28). Jha and colleagues reviewed the reports of 530 SSs and found only 1 (0.2%) spinal fracture – a thoracic compression fracture (75). In a multicenter retrospective review of the data from 2049 initial SSs in children younger than 10 years, Lindberg et al. found that 16 subjects (0.8%) had spinal fractures (76). For those children with a positive SS, the prevalence rose to 3.4% (16/471). Kleinman and colleagues reviewed the reports of SSs of 365 children less than 2 years of age that were performed in the film/screen era and found 25 spine fractures in 10 of 365 (2.7%) of cases (77).
More recently, Barber et al. reviewed the results of computed radiographic SSs in 751 children to establish the prevalence of spinal fractures, and to determine the association between spinal fractures and intracranial injury (ICI) (78). The mean age of children in the cohort was 10 months (range: 4 days to 4 years); 567 of 751 (75%) were infants (<1 year of age), 108 of 751 (14%) were between 1 and 2 years of age, and 76 of 751 (10%) were greater than 2 years old. There were 440 males and 311 females. Fourteen patients had a definite spinal fracture with a mean age of 16 months (range: 2–39 months) for a total of 22 definite spinal fractures. This prevalence of spinal fractures was 1.9% (14/751) for the total cohort, and 9.7% (14/145) for those patients with a positive SS (Table 21.2) (78). Cross-sectional or radionuclide imaging confirmed the fractures in 13 of 14 children and revealed 12 additional spinal fractures. In 5 children, spinal fractures were the only positive skeletal findings. In 10 of 14 patients, the spinal fractures were accompanied by ICI establishing that patients with spinal fractures are far more likely to have ICI than those without spinal injury (P <0.05). These findings also support the view that inflicted spinal fractures, while uncommon, are not rare. Barber et al. also noted significant age-related differences in the prevalence of spine fractures with a higher fracture rate occurring in children greater than two years of age (Table 21.3). Older children with spine fractures were more likely to have a positive SS (defined as the presence of unsuspected fracture) (78). Thisage-related difference in the occurrence of spinal fractures was also noted in the 20 center study data of Lindberg et al. (76). In children with positive SSs, 10 of 417 (2.4%) children aged younger than 24 months had spinal fractures, versus 6 of 54 (11%) children aged older than 24 months. These findings have potential implications for the approach to SS screening of children beyond infancy (see below).
| Age/ gender | Presentation | Clinical Indication | Intracranial Injury | RH | Spinal definite fracture on SS (type of fracture and projection*) | Additional fractures on SS | Additional imaging (spinal fractures**) | |
|---|---|---|---|---|---|---|---|---|
| Case 1 | 2 months/M | Neuroimaging after new focal seizures | ICI, suspected AHT | SDH (B), parenchymal injury (CT, MR) | – | T12 (BC on AP and L) | Ribs, CMLs | F18 + (T12) CT (T12) |
| Case 2 | 6 months/F | Status post-fall from couch. Skull fracture and severe ICI | Ribs fractures on chest radiograph | SDH (U), SAH, parenchymal injury (CT, MR) | + B | T11, T12 (BC on L only) | Ribs, tibia | F18 + (T11 T12) |
| Case 3 | 3 years/M | Maternal concern over multiple bruises | Multiple bruises | – (CT) | – | T7 (BC on AP only) | – | F18 + (T7) |
| Case 4 | 2 years/M | Neuroimaging after new focal seizures | ICI, suspected AHT | SDH (U), SAH, parenchymal injury (CT, MR) | + B | T4 (BC on L only) | Fibulas | F18 + and abdominal CT (T4, and add T9, T10) |
| Case 5 | 19 months/M | Neuroimaging after minor head trauma | Bruises and discrepant mechanism for ICI | SDH (U), parenchymal injury (CT, MR) | + B | T8 (BC on AP and L) | – | F18 + (T8) |
| Case 6 | 2 months/F | Neuroimaging after ALTE | Apneic episode and unexplained bruises | SDH (B), SAH (CT, MR) | + B | T3 (BC on L only),T10 (BC on AP and L) | – | F18 + (T10) And spine MR (T3, T10) |
| Case 7 | 22 months/M | Concern about a lesion in his right arm without history of trauma | Unexplained distal humerus fracture | – (CT) | – | T4 (BC on AP and L) | CML | none |
| Case 8 | 8 months/F | Transferred with diffuse bruising | Multiple bruises | – (CT) | – | L3, L4 (BC on L only) | – | Abdominal CT. Liver laceration (L3, L4, and add T12, L1, L2) |
| Case 9 | 6 months/M | Cardio-respiratory arrest | Rib fractures on chest radiograph | Tentorial SDH (CT, MR) | – | T12 (BD on AP and L), S4 (compression on L only) | Ribs, CMLs, scapula, metatarsal, and skull | Thoracic-abdominal CT. Spine MR (T12, S4, and add C4) |
| Case 10 | 15 months/M | Right leg swelling. Developmental delay | Femur fracture and social concern | SDH (B), cerebral atrophy, abnormal brain parenchyma suggestive of old injury (CT, MR) | – | L1, L2 (BC on L only) | – | BS + (L1, L2) |
| Case 11 | 8 months/F | Decreased activity. No history of trauma | Bilateral proximal femur fractures | – (CT, MR) | – | S3 (compression on L only) | Multiple long bones | MR of the sacrum (S3) |
| Case 12 | 12 months/F | Neuroimaging for altered mental status | ICI, suspected AHT | SDH (B), SAH, parenchymal injury (CT, MR) | + B | T7, T8, T9 (BC on AP and L) | Multiple long bones | Thoracic-abdominal CT (T7–T9 and add T5, T6, T10) |
| Case 13 | 32 months/F | Right hemiparesis | Multiple bruises | Tentorial SDH, SAH (CT, MR) | + U | T5 and T6 (BC on AP and L) | Isolated CCJ rib | Spinal MR (T5, T6, and add T4, T7) |
| Case 14 | 25 months/F | Status post-fall. Skull fracture and ICI | Injuries after unwitnessed fall atypical given the history. | SDH (B), SAH (CT, MR) | + U | T7 (BC on AP and L) | Tibia metaphyseal fracture explained by prior accident | F18 +, and spinal MR (T7 and add T8) |
* Radiologic projection of the skeletal survey in which the fracture was evident: AP, chest or abdomen anterior view; BC, body compression; BD, body dislocation; L, lateral view of the chest and/or the lumbar spine.
** Twelve additional spinal fractures identified on CT, MRI, or bone scan in bold.
add, additional; AHT, abusive head trauma; ALTE, apparent life-threatening event; B, bilateral; CML, classic metaphyseal lesion; ICI, intracranial injury; RH, retinal haemorrhage; SAH, subarachnoid hemorrhage; SS, skeletal survey; U, unilateral.
| Age group | Total patients | Patients with spinal fractures | Patients with +SS | Prevalence (Overall; +SS) |
|---|---|---|---|---|
| Less than 24 months | 675 | 10 | 137 (20%) | 1.5%; 7.3% |
| Greater than 24 months | 76 | 4 | 8 (10%) | 5.3%; 50% |
| Total | 751 | 14 | 145 | 1.9%; 9.7% |
+ SS, Positive skeletal survey.
As noted above, the spectrum of abuse-related spinal fractures ranges from subtle, self-limited spinal compression fractures to neurologically devastating, occasionally fatal, fracture-dislocations. The topic of inflicted spine injury receives only modest attention in the child abuse literature. This is unfortunate given the clinical significance of severe, but often occult spinal injuries, as well as the diagnostic importance of any spinal fracture – an injury which can be the only positive traumatic finding on SS (78). Therefore, a thorough discussion of the subject is essential if the imaging features of these underappreciated manifestations of child abuse are to be fully understood.
The craniocervical junction and the cervical spine
The topic of abusive injury of the craniocervical junction (CCJ) and the lower cervical spine has received scant attention in the imaging literature, despite the fact that these injuries are more likely to have clinical consequences than injuries of the sub-cervical region. There are few imaging reports that detail such injuries in living children with inflicted trauma, and thus the true incidence/prevalence of abusive injury of the CCJ and cervical spine is unknown (74). By contrast, cervical injuries identified at postmortem in fatally abused children are well documented in the forensic literature.
Inflicted injury of the cervical region is most commonly observed in conjunction with AHT, but not exclusively (17, 37, 74). Most AHT occurs in children under one year of age, and then predominantly in those less than six months of age (79). Similarly, most instances of inflicted cervical spine trauma are identified in infants, with a median age of five months (74). Although nonligamentous cervical injuries are rarely documented in abused children, when such injuries are present, the consequences may be significant and potentially life-threatening (7, 21).
There may be substantial risk to missing CCJ or cervical spine injury in the abused child. Minor injury may have little or no clinical impact, but more severe injuries may require treatment to prevent further injury, chronic myelopathy, or orthopedic deformity (21, 80, 81). If cervical spine injury is unstable, but clinically inapparent and not recognized, then ongoing repetitive spinal injury, cord compromise, pain, and kyphotic deformity may result, with the potential for significant disability and even mortality (82). Therefore, timely diagnosis of both bony and ligamentous injuries is important. Cervical spine fractures may be recognized on the SS, while potentially significant ligamentous injuries that are indiscernible on radiography are missed. Undiagnosed post-traumatic spine instability, first caused by abusive trauma, may not become evident until months after the initial traumatic event (7). Unrecognized cervical spinal injury in early infancy may lead to spasticity and be misdiagnosed as cerebral palsy.
The imaging features of inflicted CCJ and cervical spine injuries have much in common with those encountered in accident victims, and to fully comprehend this spectrum, a discussion of accidental injuries occurring in this region is appropriate. Many of the principles at work in accidental CCJ and cervical spine trauma are also applicable to inflicted injury of these regions.
It should be noted that the type, level, frequency, and outcome of cervical spine injuries in children differs significantly from those seen in adults. Most pediatric spine trauma involves the cervical region, which accounts for approximately 72% of all spinal injuries in children less than 8 years of age (83, 84). In older children the pattern of spinal injury tends to resemble that of adults (85, 86). In young children the upper cervical spine, including the CCJ, is the most common accidentally injured spinal region (67, 83, 87). Similarly, the high cervical spine is the most commonly injured region in children with inflicted spine trauma (74).
Relevant anatomy and function
The CCJ extends from the basiocciput to the second cervical interspace, and is a region that is functionally and developmentally distinct from the remainder of the cervical spine. It is composed of chondro-osseous, ligamentous, and musculotendinous structures that work in concert to provide mobility and stability to this complex functional unit (Fig. 21.2).
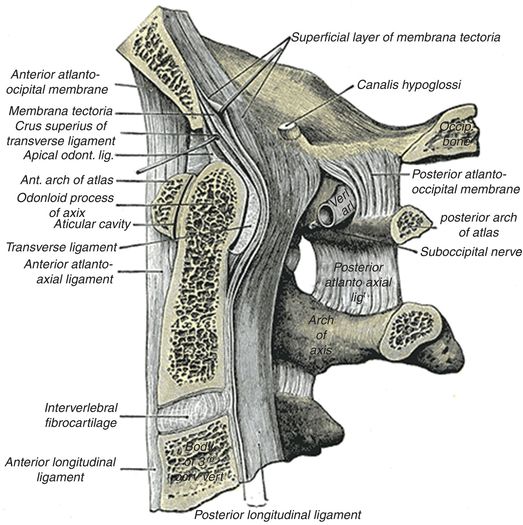
Figure 21.2 Sagittal section through the CCJ shows the normal bony anatomy and ligamentous attachments. (From Gray’s Anatomy, 20th US edn, in the public domain.)
Occipital bone and foramen magnum
The occipital bone forms the most caudal portion of the calvarium. Posteriorly, the curved part of the occipital bone below the superior nuchal line is referred to as the suboccipital region. Anteriorly, the basilar part, or the basiocciput, constitutes the inferior half of the clivus. The foramen magnum is the large midline oval aperture at the base of the skull, which transmits the medulla, membranes, arteries, and nerves; it is flanked laterally by the occipital condyles. The paired occipital condyles are the inferior facets of the occipital bone, which articulate with the superior articular facets of the atlas. The midpoint of the anterior margin of the foramen magnum is called the basion; the midpoint of the posterior margin is termed the opisthion. Many of the muscles that stabilize the atlanto-occipital and atlanto-axial joints attach to the occipital bone (Fig. 21.3).
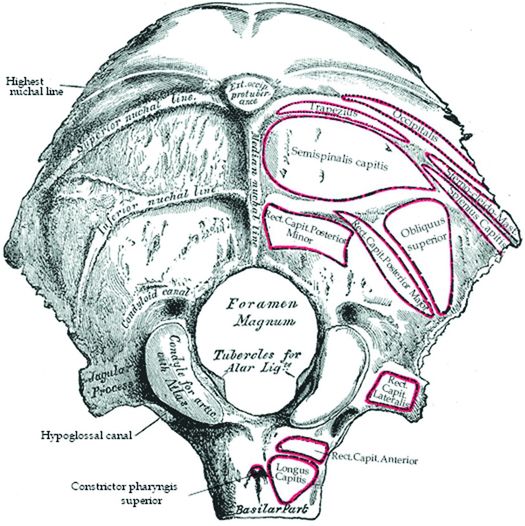
Figure 21.3 Occipital bone. Outer surface. (From Gray’s Anatomy, 20th US edn, in the public domain.)
Atlas (C1)
C1, or the atlas, is uniquely ring-shaped and does not possess a true vertebral body (Fig. 21.4). It articulates superiorly with the occipital condyles, and inferiorly with the axis by way of the odontoid process medially and the paired atlanto-axial joints laterally.
Figure 21.4 The atlas, the first cervical vertebra, viewed from above. (From Gray’s Anatomy, 20th US edn, in the public domain.)
Axis (C2) and the subaxial cervical spine
C2, or the axis, uniquely possesses a midline tooth-like bony projection called the odontoid process, which in conjunction with investing ligaments plays an essential role in constraining movement at the CCJ (Fig. 21.5). In contrast to the subaxial spine, where the pedicles lie anterior to the superior and inferior articular facets, the pedicles of C2 lie directly beneath the superior facet, while the pars interarticularis forms the narrower portion of bone between the superior and inferior facets. This anatomy will be important in the discussion of the Hangman’s fracture and its differential consideration, congenital spondylolysis of C2 (see below). The C2–3 apophyseal joints are similar to the other articulations of the subaxial cervical spine.
Figure 21.5 The axis, the second cervical vertebra, viewed from above. (From Gray’s Anatomy, 20th US edn, in the public domain.)
Ligaments
The cranium is secured to the upper cervical spine by the complex ligamentous anatomy of the CCJ. The anterior atlanto-occipital ligament extends from the inferior and anterior surface of the clivus to the anterior body of C2; it is contiguous inferiorly with the anterior longitudinal ligament (ALL) (Figs. 21.2, 21.6). Laterally, the lateral atlanto-occipital ligaments join the occiput to the atlas and extend from the lateral margin of the foramen magnum to the superolateral border of the posterior arch of the atlas and its lateral masses (Fig. 21.6). The apical and alar ligaments secure the dens of C2 to the skull base. The apical ligament is a midline structure that extends from the basion to the tip of the dens (Figs. 21.2, 21.7). The paired alar ligaments attach to the ventral and lateral surface of the odontoid process and extend superiorly and laterally to the occipital condyles and lateral masses of the atlas (Fig. 21.7). The alar ligaments prevent excessive flexion and extension, rotation, and lateral flexion (88).
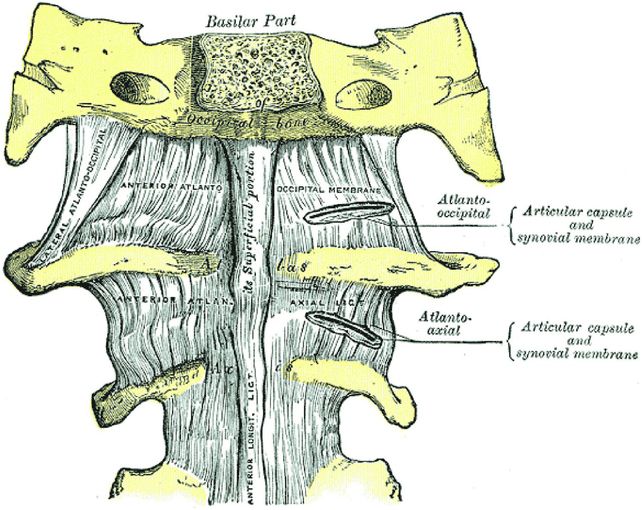
Figure 21.6 Anterior view of the CCJ shows the anterior and lateral atlanto-occipital membranes and the atlanto-axial ligament. (From Gray’s Anatomy, 20th US edn, in the public domain.)
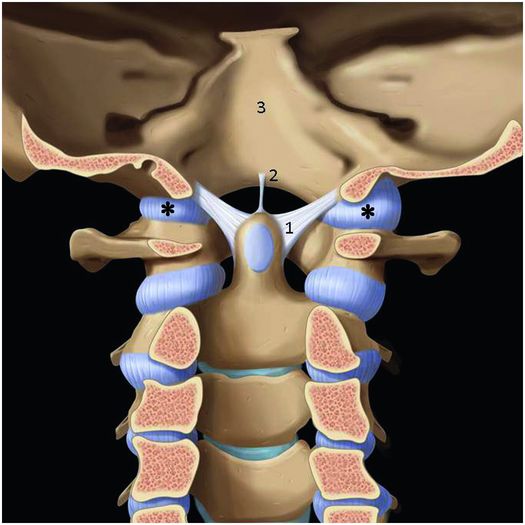
Figure 21.7 Anterior view of the apical and alar ligaments. 1. Alar ligament. 2. Apical ligament. 3. Basiocciput. * Capsular ligament. (Used with permission from Amirsys Publishing, Inc.)
The cruciate ligament is cross-shaped, formed as a vertical and a horizontal band that secures the odontoid process to the atlas and skull base (Fig. 21.8). The vertical band of the cruciate ligament extends from the basion to the body of the axis and lies between the apical ligament and the tectorial membrane (see Fig. 21.2). The transverse ligament, the most well-developed portion of the cruciate ligament, passes posterior to the dens and attaches to the lateral masses on each side of the atlas (Figs. 21.8, 21.9). Together with the anterior arch of C1, the transverse ligament forms a fibro-osseous ring around the dens that stabilizes the joint and allows for a pivoting motion between the two bones. The transverse ligament prevents anterior dislocation of the atlas on the axis during flexion. Failure of the transverse ligament is rare in young children, in whom the dental synchondrosis of C2 is more likely to fail before the transverse ligament.
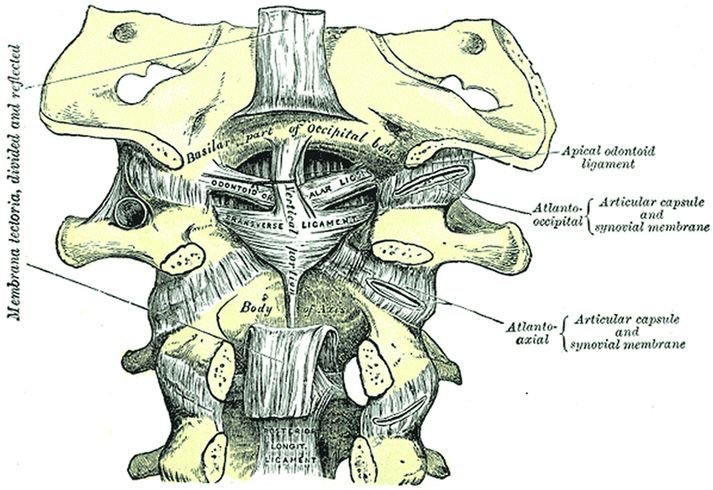
Figure 21.8 Tectorial membrane, cruciform and alar ligaments, posterior view. The tectorial membrane is transected. (From Gray’s Anatomy, 20th US edn, in the public domain.)
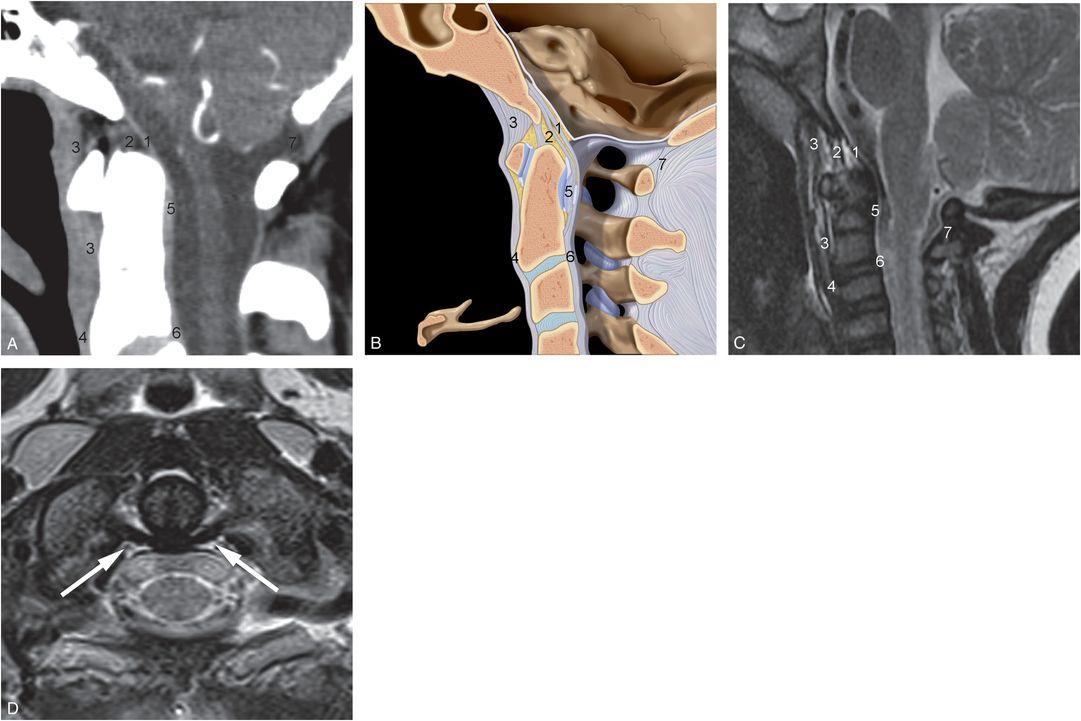
Figure 21.9 Ligaments of the CCJ. A, Sagittal post-contrast reformatted image of a cervical CT. B, Sagittal illustration. C, Sagittal T2WI of another patient shows: (1) tectorial membrane, (2) apical and cruciate ligaments, (3) anterior atlanto-occipital ligament, (4) Anterior longitudinal ligament, (5) transverse ligament, (6) posterior longitudinal ligament, and (7) posterior atlanto-occipital ligament. D, Axial T2WI image of C2 of another patient demonstrates the normal, hypointense transverse ligament (arrows) dorsal to the dens. (B, Used with permission from Amirsys Publishing, Inc.)
The alar ligaments and the transverse band of the cruciform ligament are considered the most important ligaments providing craniocervical stability (89). The C1–2 capsular ligaments function primarily to restrict axial rotation (90) (Figs. 21.7–21.10). Unilateral transection of the capsular ligament results in increased range of motion on the opposite side.
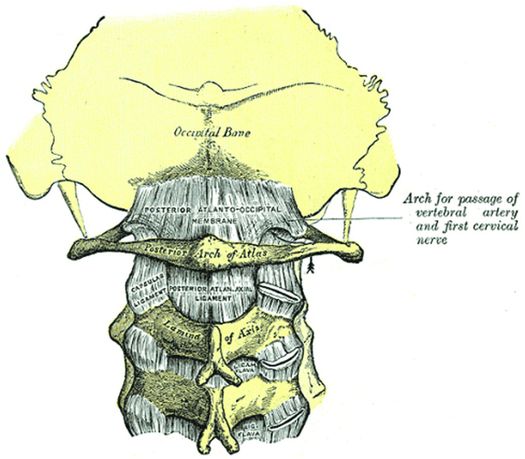
Figure 21.10 Posterior view of the CCJ shows the posterior atlanto-occipital membrane, atlanto-axial ligament, and capsular ligaments. (From Gray’s Anatomy, 20th US edn, in the public domain.)
The tectorial membrane is tightly adherent to the clivus. Superiorly, it attaches to the clivus and jugular tubercles approximately at the level of the spheno-occipital synchondrosis. Inferiorly, it extends to the base and body of C2 and is contiguous with the posterior longitudinal ligament (Figs. 21.2, 21.9).
Various opinions regarding the role of the tectorial membrane in maintaining CCJ stability are expressed in the literature, including those of Harris et al. (91) and Krakenes et al. (92), who believe that the tectorial membrane plays an important role in maintaining CCJ stability, and Tubbs et al. (93) who suggest that the contribution of the tectorial membrane to CCJ stability is minimal and that the main function of the membrane is to protect the cervical spinal cord in flexion. In this position, the tectorial membrane stretches over the odontoid process and prevents it from moving posteriorly, thereby limiting impingement of the dens into the cervical canal (93).
Posteriorly, the CCJ does not have well-developed ligamentous supporting structures. The posterior ligamentous support of the CCJ is provided by the posterior atlanto-occipital ligament, which extends from the anterior surface of the posterior ring of C1 to the posterior foramen magnum. Inferiorly, it is contiguous with the ligamentum flavum. The ligamentum flava connect successive laminae of adjacent vertebrae in the cervical spine. Posteriorly in the midline, the interspinous ligaments connect the spinous processes from their roots to their apices. The ventral surface of the interspinous ligament meets the ligamentum flavum and the ligament blends dorsally with the supraspinous ligament. The midline nuchal ligament extends from the external occipital protuberance and median nuchal line to the posterior tubercle of C1 and to the spinous processes of the cervical vertebrae. The nuchal ligament is the cranial continuation of the interspinous and supraspinous ligaments and forms a midline septum between the muscles on either side of the neck. This ligament limits flexion of the head and neck.
Muscles
The muscles of the CCJ are organized in three different layers. The most superficial layer is formed by the trapezius and sternocleidomastoid muscles. The intermediate layer is composed of the semispinalis and splenius capitus muscles. The deepest layer consists of the rectus capitis posterior major and minor muscles, and the inferior and superior oblique capitis muscles.
Intraspinal contents
An in-depth discussion of meninges and the spinal cord is beyond the scope this chapter, and the relevant anatomy of these tissues will be addressed below in the individual discussions of injuries of these tissues.
Injury spectrum
The varied spectrum of imaging findings observed in children with inflicted CCJ and cervical spine injury include: (1) pre- and posterior cervical soft tissue edema and hemorrhage; (2) ligamentous strain and disruptions; (3) fractures, dislocations, and disk herniations; (4) subdural hematomas (SDHs) and epidural hematomas (EDHs); (5) cervicomedullary and cervical cord injuries; and (6) retroclival hematomas and tectorial membrane disruptions.
Injuries of the skeleton and supporting structures
Mechanisms of injury
Proposed mechanisms for injuries of the CCJ and cervical spine are complex and varied, and most studies have focused on the biomechanics entailed in bony and ligamentous disruptions. These mechanisms are also implicated in some of the injuries to the spinal cord and meninges (see below). While cervical spine injury is uncommon in young children, when it does occur, it usually affects the CCJ (67, 94–96). The infant cervical spine is significantly more mobile and deformable than that of older children and adults. This characteristic hypermobility arises from unique anatomical and biomechanical properties of the developing spine that render the CCJ inherently less stable. The increased mobility of the infant cervical spine offers less protection to the spinal cord, but it protects the spinal column from trauma that otherwise might result in a bony fracture. This may explain the relatively low incidence of spinal column fractures in young children with cervical spine trauma.
Various anatomical and biomechanical features of the developing pediatric spine may contribute to the vulnerability of the CCJ and account for the increased intersegmental spinal mobility. These include: the large size of the child’s head relative to the size of the neck; underdeveloped nuchal musculature; the ability of ligamentous and capsular/synovial membranes to stretch, permitting spinal elongation without disruption; anterior cervical vertebral body wedging, which enhances flexion and facilitates anterior translation of cervical vertebral bodies; the presence of neurocentral synchondroses and ring apophyses of vertebral body end plates, which are the cartilaginous growth plates of cervical vertebral bodies; the increased height of cervical disk material relative to vertebral body bone height (97, 98); horizontally oriented facet joints, which facilitate vertebral sliding (99); undeveloped uncinate processes (which are absent in children <10 years of age and normally protect the spine against lateral and rotational forces); horizontally oriented atlanto-occipital joints; and small, flat occipital condyles (98, 100–103).
Other features that contribute to hypermobility of the young spine include the ability of the posterior spinal ligaments to stretch with flexion; the configuration of the underdeveloped spinous and transverse processes of the cervical vertebrae, which anchor the stabilizing spinal musculature; and the underdeveloped paraspinal musculature that serves to reinforce the spine. Spinal mobility may be further augmented by the horizontal rather than vertical orientation of the alar ligaments; deficiency of the apical ligament, which may be hypoplastic or absent; and the cartilaginous compostion of the apical portion of the dens in the infant spine, which normally serves to anchor the alar, apical, and transverse ligaments and may be excessively flexible (102). These factors result in hypermobility of the CCJ, which is particularly evident in infants, in whom considerable sliding of the occipital condyles relative to the C1 articular processes can be demonstrated at fluoroscopy and on postmortem examinations (102).
These anatomic features that are so distinctive in the immature pediatric spine evolve with time as ligaments gain tensile strength; bones mature in size and shape; mature calcified bone replaces cartilage; muscles mature; and body proportions change such that the head becomes proportionally smaller relative to the torso. These changes shift the propensity of injury levels in spinal trauma from the CCJ, as seen in infants and toddlers, to the C3–4 level by age 6, and then to the C5–6 level by the age of 8–9, at which time injury patterns start to parallel those of adults (98). Experimental studies suggest that most displacement in the neck of young infants occurs in the upper cervical region (104–109). To date, there are no reports in the literature of human biomechanical data that define failure or injury thresholds of the pediatric cervical spine from bending. This is unfortunate as cervical hyperflexion and hyperextension are likely important injury mechanisms in infants with abusive craniospinal injury. In addition, neck rotation, combined with flexion or extension, as well as rebound rotation following head impact may be contributing factors to cervical spine injury in cases of abuse (97, 98).
Although the above factors lay the groundwork for understanding inflicted cervical injury, as with many other abusive injuries, mechanisms are often based on inferences drawn from similar anatomical alterations occurring with accidental trauma. On occasion, a confession or witnessed event provides direct evidence of the mechanism of injury in cases of abuse. A case in point is the hangman’s fracture (bilateral fractures of the pedicles of C2), a rare but important injury in childhood (9, 36, 73, 110, 111). Several cases of hangman’s fractures in children have been attributed to abuse (9, 11, 26, 73, 112). These fractures are generally associated with a hyperextension mechanism of injury, as occurs with falls or motor vehicle accidents (MVAs). McGrory and Fenichel reported a four-month-old infant with a hangman’s fracture that occurred secondary to shaking (36). In this case, the mother reported forcibly shaking the child by the shoulders resulting in a period of apnea and cyanosis. Kemp et al. also described shaking as the mechanism of cervical spine injury (confirmed by confessions of the perpetrators or statements of witnesses) in three cases of abuse (74). Curphey and associates described a different mechanism of injury in a traumatized 3-week-old infant with a fracture-dislocation at C2–3 (42). The father confessed to having carried out repeated beatings of the infant because of continual crying. On the day of the baby’s death, the father admitted to squeezing and twisting the child’s neck such that he heard a “snapping” sound, suggesting a mechanism of lateral neck flexion and/or torsion. In a case from the authors’ institution (see Figs. 21.14, 21.50), an infant with a C4 vertebral body compression fracture also had a T12 fracture-dislocation and a sacral fracture. The soft tissue injury overlying the sacral fracture suggested an axial-loading mechanism of injury such as slamming the child onto the buttocks.
Injury patterns
Ligamentous strain and disruptions
Most of the CCJ and cervical spine injuries in abused children are ligamentous, rather than osseous, and they frequently coexist with severe intracranial pathology, in particular bilateral hypoxic ischemic injury (HII) (37, 66). Numerous measurement criteria aimed at identifying ligamentous injury have been developed for radiographic assessment of the CCJ such as the Power’s ratio (113). While these methods often identify severe cervical spine injuries, the approach is limited because of the indirect nature of these techniques in which ligamentous disruption of the CCJ is inferred rather than visualized. Additional limitations include the assumption that accepted ranges for normal measurements based on radiographic data and adult criteria can be applied to multi-detector CT (MDCT) and to children without modification (114). In a report by Sun et al. that examined a cohort of children with cervical spine trauma, only the most severe cases of CCJ injury as detected on MRI had abnormal radiologic measurements, while children with milder injuries had normal measurements (67). Thus, mild to moderate CCJ injuries can be missed if imaging is limited to radiographs (Fig. 21.11) (115). Occiput–C1 and C1–2 dislocations or subluxations with widening of the facets can be identified on radiographs, CT, and MRI. The normal measurements defining these relationships are often different in children than adults, and thus, where appropriate, pediatric reference values should be used in the interpretation of craniocervical MDCT images (114). MRI may also identify fluid accumulation between facets related to facet injury (Fig. 21.12).
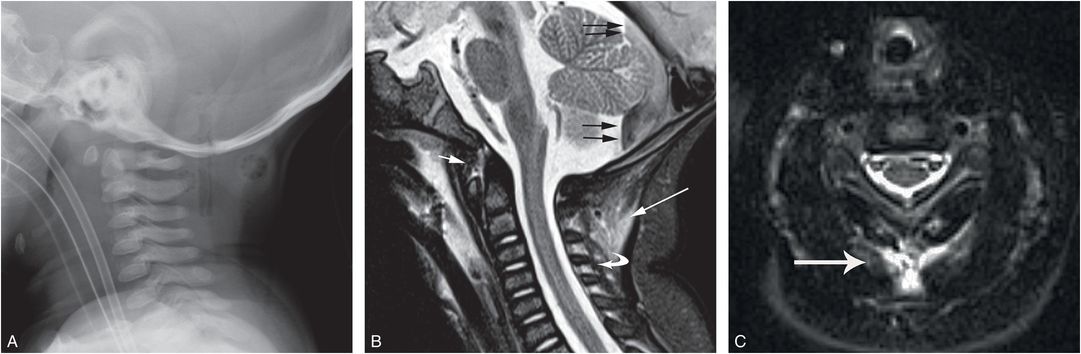
Figure 21.11 Deep cervical soft tissue and ligamentous injury. Four-month-old with vomiting and respiratory distress, who was reportedly dropped by the father while walking down stairs. Imaging showed hypoxic ischemic injury, SDH, RHs, and no skull fracture. SS revealed a CML of the distal tibia. A, Lateral radiograph from the SS was interpreted as normal. B, Sagittal STIR image shows edema within deep cervical soft tissues (long white arrow), interspinous ligament (curved arrow), and pre-cervical (short white arrow) soft tissues. Note the posterior fossa SDH with a fluid–fluid level (black arrows). C, Axial STIR image at the C3 level shows edema within posterior paraspinal soft tissues and interspinous ligaments (white arrow).
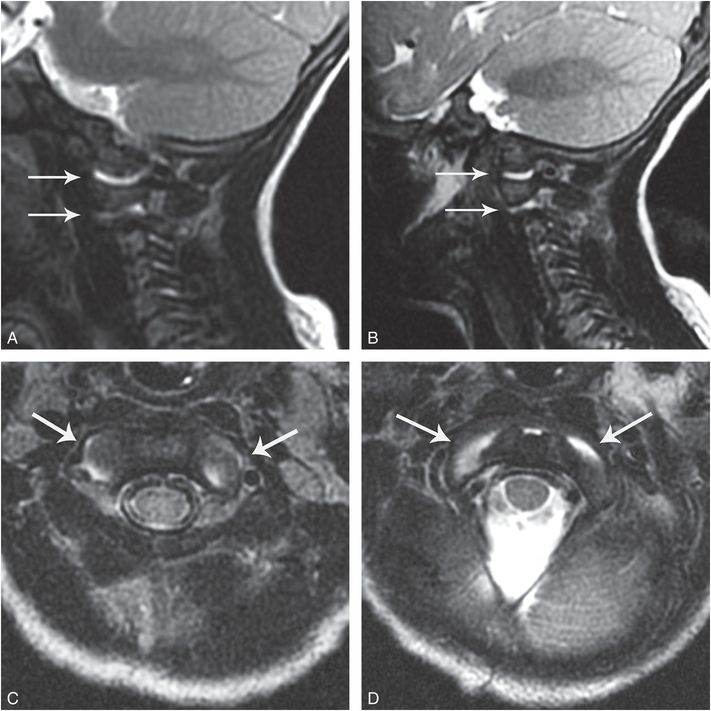
Figure 21.12 Occiput–C1 and C1–2 injury. Six-month-old with five days of respiratory congestion followed by the acute onset of respiratory distress. Imaging showed a skull fracture but no HII or SDH. SS showed multiple fractures including CMLs and cervical vertebral body fracture and a T12 fracture-dislocation. (See same patient in Figs. 5.67; 21.14; 21.31; 21.50.) A, B, Sagittal T2WIs show mild distraction and fluid within the atlanto-occipital and atlanto-axial joints bilaterally (arrows), consistent with injury. C, D, Axial T2WIs with fat saturation (FS) show fluid within the atlanto-occipital and atlanto-axial joints (arrows), respectively.
Fractures, dislocation, and disk herniations
Although bony injuries of the CCJ and cervical spine are well described in severe accidental trauma in infants and young children, they are rarely reported in cases of abuse (17, 20, 21, 39, 67, 74, 116, 117). When CCJ injury is present, it may be evident as a fracture involving the occipital squama, occipital condyles, or foramen magnum (see Chapter 17), avulsion of the anterior arch of C1, compression fracture of the posterior arch of C1, odontoid fracture, traumatic C2 spondylolisthesis (hangman’s fracture), C2 teardrop fracture, vertebral end-plate fracture, and subluxation/dislocation or distraction injuries of the atlanto-occipital and atlanto-axial joints. A case of inflicted CCJ injury was reported by Akbarnia who described a 7-year-old boy with anterior subluxation of C1 on C2 in addition to multiple other injuries (39). Additionally, Feldman and others reported a case of a 24-day-old abused child with atlanto-occipital dislocation and atlanto-axial subluxation (20, 21). MRI revealed narrowing of the upper cervical spinal canal and T2 signal prolongation within the medulla and upper cervical cord. Multiple skeletal injuries, a liver laceration, a SDH, and HII were also present. Imaging pointed to disruption of the strong ligamentous complex of the CCJ. Oral and others described a fracture through the synchondrosis of C2 in a 4-year-old with developmental delay and hypotonia (31). The babysitter admitted to slamming the child onto a bed, but further details were limited. Radiography revealed an anteriorly angulated odontoid process, and CT confirmed the displaced fracture through the base of the odontoid (Fig. 21.13).
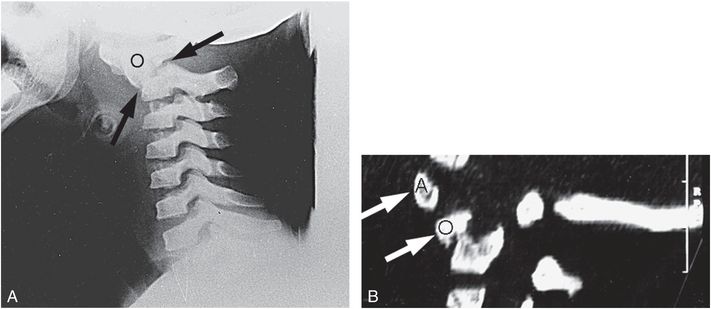
Figure 21.13 C2 synchondrosis fracture. Four-year-old child with developmental delay and chronic hypotonia with acute onset of irritability and transient difficulty walking. A, Lateral view of the cervical spine reveals a fracture (arrows) through the synchondrosis between the odontoid process and the body of C2 with anterior displacement and angulation of the odontoid fragment (O). B, Parasagittal CT reformat shows anterior displacement of the anterior arch of C1 (A) and the odontoid fragment (O). According to the babysitter’s admission the child was thrown onto a bed from a distance of 1–2 ft. (With permission from Oral R, Rahhal R, Elshershari H, Menezes AH. Intentional avulsion fracture of the second cervical vertebra in a hypotonic child. Pediatr Emerg Care. 2006;22:352–4.)
Cervical vertebral body fractures are uncommon in child abuse and reported cases are usually associated with posterior element fractures and/or ligamentous instability (see below). In contrast to simple thoracic or lumbar vertebral body compression injuries, cervical fractures are more likely to be associated with neurologic findings. Isolated cervical vertebral body fractures may result in bony retropulsion and narrowing of the cervical spinal canal. Feldman and associates reported a two-month-old infant with multiple skeletal injuries and a SDH who had diminished upper extremity movement noted four days after admission (see Table 21.1) (21). MRI demonstrated posterior medullary hemorrhage, C4 vertebral body marrow edema with bony retropulsion, and narrowing of the adjacent cervical spinal canal. There were no reported corresponding radiographic abnormalities. Thomas and associates described a burst fracture of the body of C3 in a 9-week-old infant presenting with hypotonia and no spontaneous arm movements (30). MRI demonstrated loss of C3 vertebral body height which was associated with a retropulsed intraspinal bone fragment and cord compression. Cervical vertebral fractures can also occur without evidence of posterior element or ligamentous injury, as noted in a 6-month-old abused infant with a fracture of the C4 vertebral body with bony retropulsion (Fig. 21.14). There were no associated neurologic findings, despite an accompanying severe T12 fracture-dislocation and sacral injury. Cervical vertebral body fractures may be associated with prevertebral calcifications (see Fig. 22.47) (118).
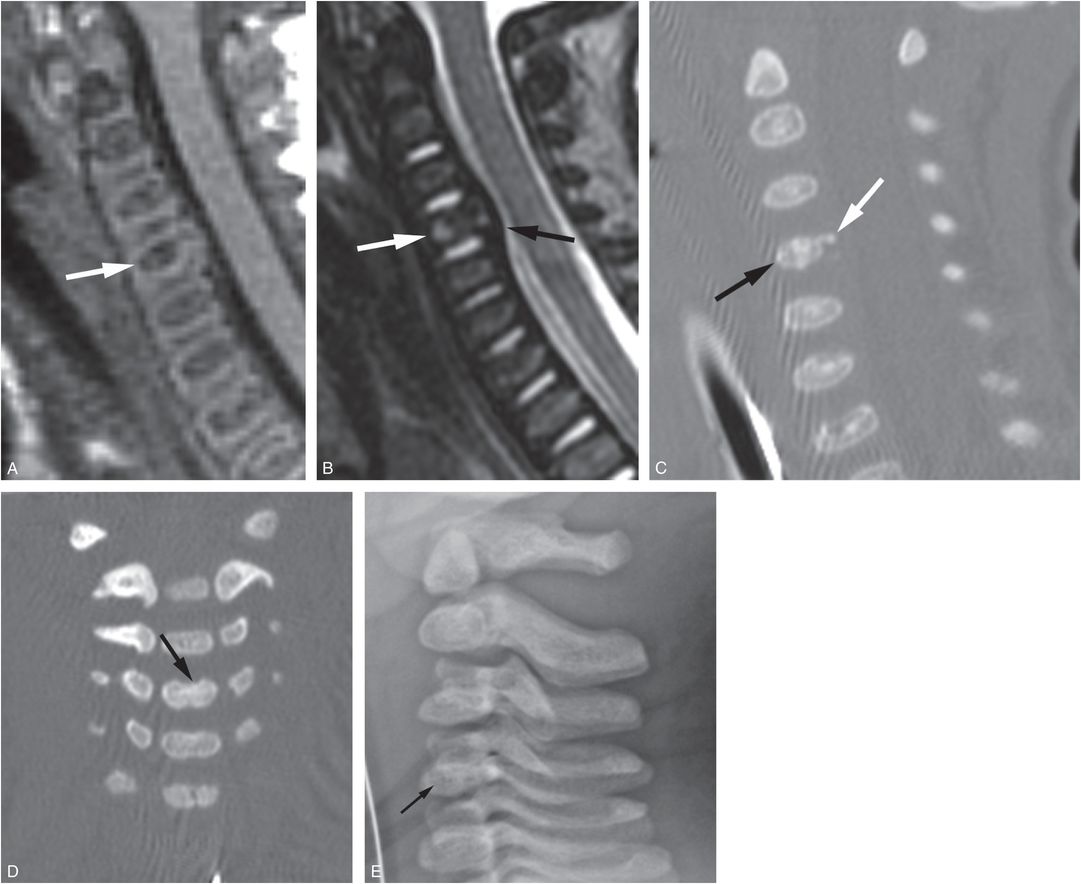
Figure 21.14 Cervical vertebral body compression deformity. Six-month-old with respiratory distress, T12 fracture-dislocation and multiple additional fractures. (See same patient in Figs. 5.67, 21.12, 21.31, 21.50.) A, B, Sagittal T1W and T2W images of the cervical spine demonstrate compression deformity of the C4 vertebral body (white arrows) with adjacent narrowing of the thecal sac (black arrow). The posterior longitudinal ligament appears intact. C, D, Subsequent sagittal and coronal reformats of the cervical spine CT demonstrate deformity of the C4 vertebral body (black arrows) with a retropulsed osseous fragment (white arrow) corresponding to the extradural mass effect. The lateral view of the cervical spine (E) from the SS was originally reported as negative, but in fact revealed a mild vertebral body compression deformity (arrow).
Hangman’s fracture
The hangman’s fracture is also known as a traumatic spondylolysis of the axis (Fig. 21.15) (9, 11, 36, 73, 110–112, 119). As the pedicles of C2 lie inferior to the atlanto-axial articulation and anterior to the C2–3 apophyseal joints, the fracture is actually through the pars interarticularis. While these fractures are considered unstable injuries, some patients may have no associated neurologic deficits. Radiographs may reveal a vertical lucency just posterior to the body of C2 (Fig. 21.15A). Most of these fractures are associated with spondylolisthesis, and thus the bony fragments are usually separated by several millimeters. The margins may be well defined without sclerosis, even when the injury is old. CT further characterizes the nature of the fracture (Fig. 21.15B). Thin axial sections and multiplanar reformatted images will define the fracture margins, the degree of anterior slippage of the body of C2 relative to C3, the extent of canal stenosis, and evidence of healing. MRI may further determine whether canal compromise results in cord compression, and will identify any associated spinal cord injury (Fig. 21.15C). Flexion and extension views are important components of the work-up and may influence orthopedic management (Fig. 21.15D). These views, however, should be obtained with caution and under careful medical supervision. The major differential consideration for a hangman’s fracture is a primary (congenital) spondylolysis of C2 (see below) (110, 111).
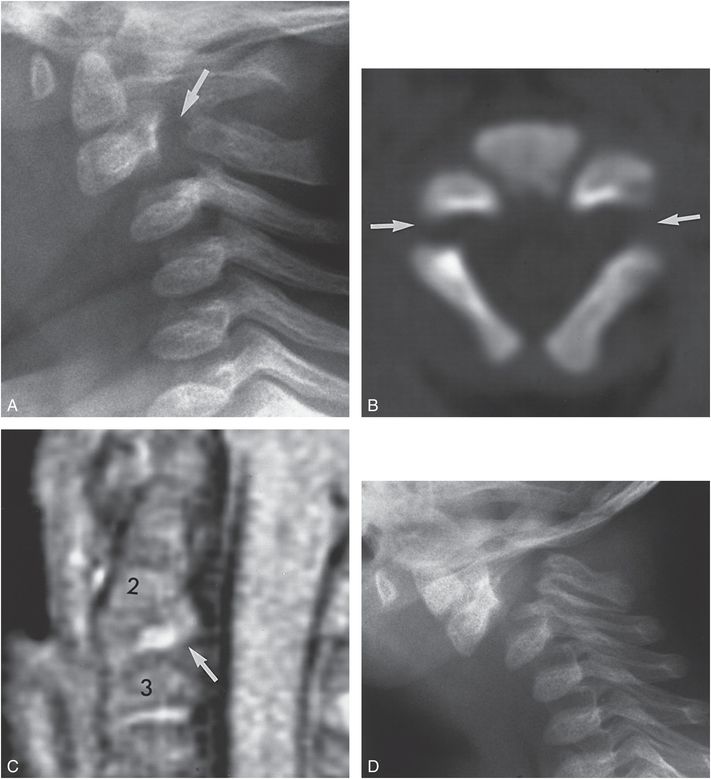
Figure 21.15 Hangman’s fracture in a six-month-old infant with multiple inflicted injuries but without signs or symptoms referable to the cervical spine. A, Lateral view of the cervical spine from the initial SS demonstrates a fracture through the pedicles of C2 (arrow). The body of C2, the odontoid, C1, and the skull are all displaced anteriorly with respect to the posterior arches of C2 and C3. B, An axial CT image shows bilateral pedicle defects (arrows) with greater separation on the left. The bony margins are smooth and there is no evidence of callus or reactive bone. C, PD MRI demonstrates widening of the C2–3 interval, with anterior displacement of C2 on C3. There is abnormally increased signal between C2 and C3 (arrow) that extends into the epidural soft tissues and is probably related to hemorrhage and extruded disk material. Despite displacement at C2–3, no deformity of the thecal sac or spinal cord injury is evident. D, Lateral view of the cervical spine in flexion obtained two months after the initial injury shows increased subluxation of C2 on C3 without evidence of healing. CT showed no evidence of healing. A bony fusion was performed. (From Kleinman PK, Shelton YA. Hangman’s fracture in an abused infant: imaging features. Pediatr Radiol. 1997;27:776–7.)
Hyperflexion fracture-dislocation
The constellation of radiographic findings associated with severe hyperflexion injuries is well described with accidental injuries in older children and adults (119). The features are similar in cases of abuse, but since the precise anatomic alterations are more difficult to assess radiographically in infants and small children, the full extent of the injuries will not be appreciated until cross-sectional imaging studies have been performed (Figs. 21.16, 21.17). With severe hyperflexion of the neck, there is disruption of the posterior ligamentous complex, which leads to subluxation of the apophyseal joints. Varying degrees of slippage may occur, ranging from subluxation to perched facets, to frank dislocation with locking of the inferior articular facet in front of the subjacent superior articular facet. More severe injuries may be associated with fractures of the displaced vertebral body as well as of the subjacent vertebrae (16).
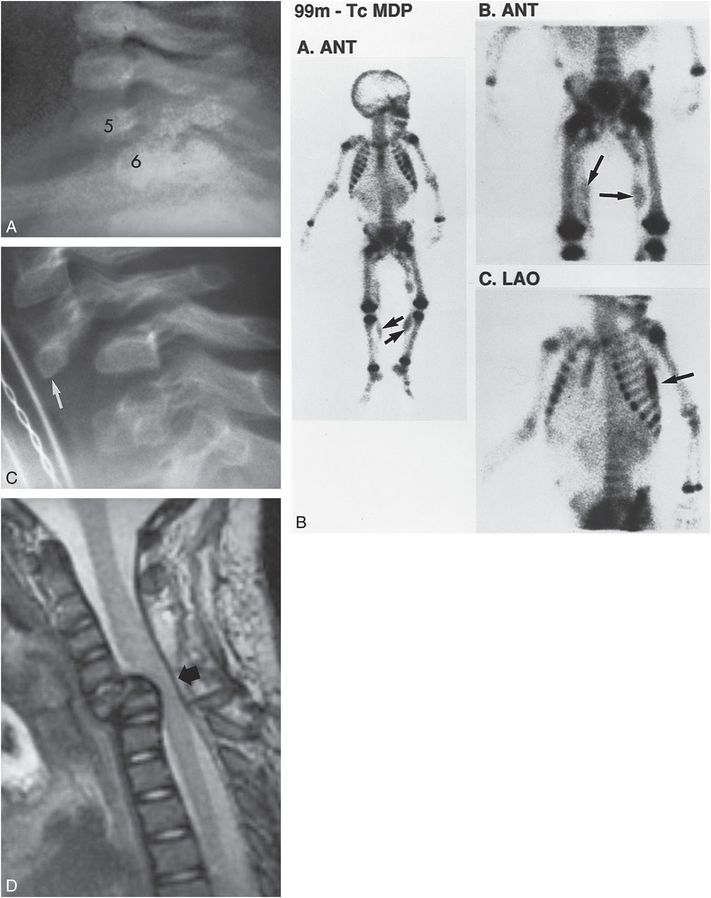
Figure 21.16 Fracture-dislocation of the cervical spine. A, Lateral radiograph of the cervical spine from the SS in a three-month-old abused twin infant shows suboptimal assessment of the lower cervical region. There is a suggestion of anterior displacement of C5 on C6. B, Three views from the 99mTc bone scan demonstrate multiple areas of abnormal activity consistent with injury (arrows), but there is no evidence of a cervical spine fracture-dislocation. C, Lateral cervical spine radiograph performed five months later demonstrates marked anterior dislocation of the apophyseal joints at C5–6. Note the deformity of the body of C5, consistent with remote fracture (arrow). D, T2W sagittal MRI at the same time as C shows marked narrowing of the AP dimension of the spinal canal with spinal cord compression (arrow). (With permission from Rooks VJ, Sisler C, Burton B. Cervical spine injury in child abuse: report of two cases. Pediatr Radiol. 1998;28:193–5.)
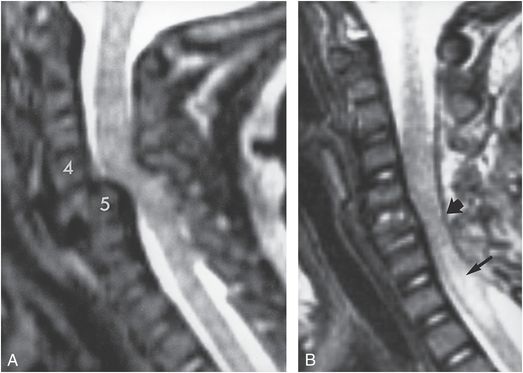
Figure 21.17 Cervical spine fracture-dislocation in the three-month-old twin sister of the infant shown in Fig. 21.16. Plain radiographs demonstrated a fracture-dislocation at C4–5 A, T2W sagittal MRI demonstrates severe displacement of C4 on C5. There is marked decrease of the AP dimension of the spinal canal. B, T2W sagittal MRI after spinal reduction shows relatively normal alignment of the vertebral bodies. However, there is atrophy of the spinal cord at the level of the injury (thick arrow) and intramedullary high signal intensity below this level consistent with syrinx or myelomalacia (thin arrow). (With permission from Rooks VJ, Sisler C, Burton B. Cervical spine injury in child abuse: report of two cases. Pediatr Radiol. 1998;28:193–5.)
With bilateral perched or locked facets, there is significant narrowing of the spinal canal. MRI in axial and sagittal planes is essential in such cases to evaluate for cord compression (Figs. 21.16, 21.17). Acutely, MRI may reveal paraspinal soft tissue injury; intraspinal SDH or EDH; spinal cord injury; and delayed MRI may demonstrate the sequelae of prior cord injury, such as myelomalacia, cord atrophy, or post-traumatic syrinx (Fig. 21.17B).
True cervical spine subluxation should not be confused with a mild degree of vertebral displacement known as pseudosubluxation, which occurs in normal children and those with muscular spasm of the cervical spine (120). Typically, this finding is most conspicuous at the C2–3 level, where pseudosubluxation may be misinterpreted as a hyperflexion injury. Children restrained on trauma boards and with cervical collars frequently show several millimeters of displacement at this level, and the finding should not be misinterpreted as abnormal.
Extra-axial collections
In children with abusive injuries, SDH or EDH may be present within the spinal canal. EDHs likely reflect localized spinal injury, whereas spinal SDHs, in the absence of additional findings suggesting spinal injury, likely represent inferior run-off of blood and/or cerebrospinal fluid (CSF) from posterior fossa collections (67). Although these lesions often point to ICI (see below), when spinal SDH is unassociated with posterior fossa subdural blood, an occult spinal injury should be considered.
Spinal EDH
Most spinal EDHs in the pediatric population are spontaneous in nature, whereas few develop secondary to trauma (121–125). Occasionally an EDH is observed following diagnostic lumbar puncture (LP). In such cases, these collections are most commonly seen in the thoracic and lumbar spinal regions (126). Although the etiology is unknown, epidural bleeding likely results from direct vessel wall injury or rupture of thin-walled veins that form the rich epidural venous plexus within the cervical spine (121, 126–128). Rutty et al. have suggested that spinal EDHs observed in children at autopsy with no additional pathology to account for the finding may represent postmortem artifact (129), while others have challenged this assertion (130).
Although CT or MRI images of inflicted cervical spine EDHs are lacking from the literature, several forensic studies have reported these collections in the context of fatal abusive injury. Hadley et al. reported the postmortem findings in 6 children under 14 months of age with abusive head injury: 5 of the 6 children had cervical EDHs (131). Saternus et al. reported 3 fatal cases of abuse in children less than 2½ years of age, and noted a 15-month-old with thin EDHs in the upper cervical region and at the cervicothoracic junction (117). Geddes et al. observed epidural blood within the upper cervical spine in 3 of 53 children with fatal AHT (132). Oehmichen et al. examined 18 children under 1 year of age who died of AHT and found lower cervical spine EDHs in 4 of 11 (36%) infants whose cervical spines were examined (133). In an autopsy series of 41 children with AHT and neck injuries reported by Brennan et al., epidural, subdural, or intradural hemorrhages were seen within the cervical spine in 24 (59%) children, but the authors offered no further details in regard to the epidural collections (134). In a study by Molina et al. examining 101 children under 5 years of age who died from inflicted blunt force trauma, 2 children had neck injuries; 1 of these was a 14-month-old who had a cervical EDH associated with atlanto-occipital dislocation and medullary contusion (135).
Imaging
In lieu of reported published images of abusive spinal EDH, it is necessary to draw inferences from the features of spinal EDHs sustained with obstetric and accidental trauma. Cervical spine EDHs are observed in neonates with birth-related trauma and cervical cord injury (Fig. 21.18) (136). MRI is the imaging modality of choice for identification of cervical EDHs, especially for small collections. Even with MRI assessment, cervical EDHs related to trauma are rarely observed. Possible explanations for this include: (1) delay in obtaining spinal MRI, thus allowing an EDH to resorb by the time imaging is performed (137); and (2) MRI technical factors that limit the ability to detect small epidural collections.
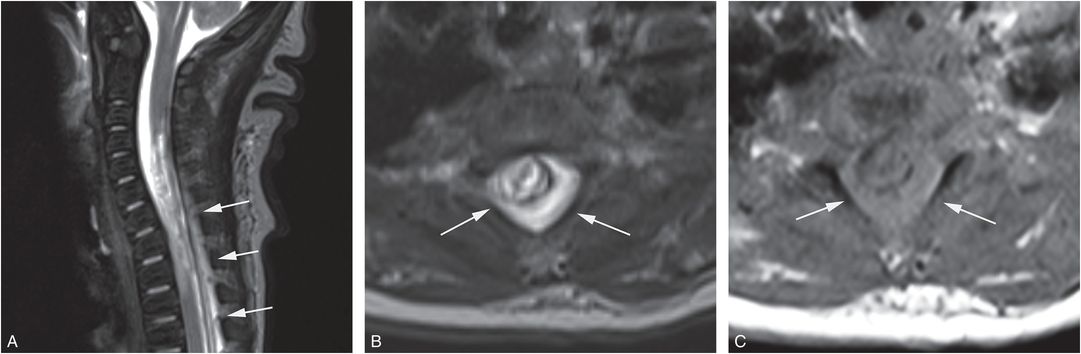
Figure 21.18 Spinal EDH. Newborn with cervical spine trauma related to a difficult birth. A, Sagittal T2WI shows spinal cord hemorrhage and edema and a posterior EDH extending from C5 into the thoracic region. B, C, Axial T2W and T1W images show the circumferential spinal EDH (arrows) with abnormal bright and intermediate signal, respectively, within the epidural space.
Spinal SDHs
The prevalence of spinal SDHs associated with AHT is estimated to lie at between 44 and 63% (131, 132, 134, 138, 139). They are less often reported in children with accidental head trauma (AccT) (67, 138).
Pertinent anatomy and mechanisms of injury
Unlike the supratentorial subdural space, no major vessels or bridging veins traverse the spinal subdural compartment (140). The spinal subarachnoid space (SAS) contains avascular structures (140), and radicular arteries and veins traverse the spinal dura via the spinal nerve sheaths. Therefore, the cause of intraspinal SDHs likely differs from that of its intracranial counterpart. Proposed mechanisms include: distal redistribution of intracranial subdural blood into the more dependent spinal compartment; hemorrhage from vessels within nerve root sleeves and along ventral and dorsal nerve roots with subsequent bleeding into the subdural space; and rupture of spinal vessels secondary to indirect injury or sudden increases in intra-abdominal pressure (67, 138, 141–143). In one case report of a child with AHT and a spinal SDH that was surgically evacuated, an actively bleeding lacerated radicular vein adherent to the arachnoid membrane was identified as the cause of bleeding. In this child hemorrhage into the subdural space occurred through a rent in the arachnoid membrane (35).
Spinal SDHs have long been identified in forensic studies of children with fatal abusive injuries (129, 131, 134, 144–146), but have only recently come to clinical attention with imaging (138, 139). In a series of eight children with AHT and spinal SDHs described by Koumellis et al., all children were managed conservatively and no cord abnormalities were seen on follow-up imaging (139). Similarly, in a larger series of children with AHT and spinal SDHs reported by Choudhary et al., all 31 children with spinal subdural collections were managed conservatively, including 2 patients with symptoms referable to the spine (138). The authors found no long-term complications referable to initial spinal cord compression on follow-up. Gruber and Rozzelle. evacuated a spinal SDH in a four-month-old child with AHT, which resulted in clinical improvement of symptoms referable to the spinal cord (35). It should be noted that spinal SDHs may occur following a diagnostic LP (126).
Imaging
In 1997 Feldman et al. compared imaging findings on cervical spine MRIs with postmortem findings in 5 children with AHT (146). At autopsy one child had a thin cervical spinal SDH in continuity with an intracranial SDH that was not detected by MRI. Gruber and Rozzelle’s case had lower extremity weakness and sustained clonus and a spinal MRI depicting a thoracolumbar SDH causing compression and displacement of the cord (35). In a series by Soto-Ares et al., eight children with suspected AHT, intracranial SDHs, and spinal MRIs were reviewed (147). Their findings included a two-month-old boy with an extensive thoracic and lumbar extra-axial hematoma that was described as epidural in location, although the images suggested that the hematoma was located within the subdural space.
As noted above, it is likely that the spinal SDHs in some cases of abuse had tracked from the posterior fossa into the more dependent spinal compartment (Figs. 21.19–21.21). Thus, the identification of a spinal SDH may serve as a marker of head injury, and should not necessarily be presumed to represent spinal trauma. Several imaging observations support this proposition: (1) the similarity between the signal intensity and/or density of the subdural collections within the posterior fossa and those within the spinal canal (Figs. 21.19, 21.20); (2) the continuity observed on imaging between posterior fossa and spinal SDHs (Figs. 21.19, 21.20); (3) the temporal relationship between posterior fossa SDHs that can decrease in size with subsequent appearance of a spinal SDH; and (4) the frequent observation of transient postoperative spinal subdural collections in children who have undergone posterior fossa surgery (138, 139, 148, 149).
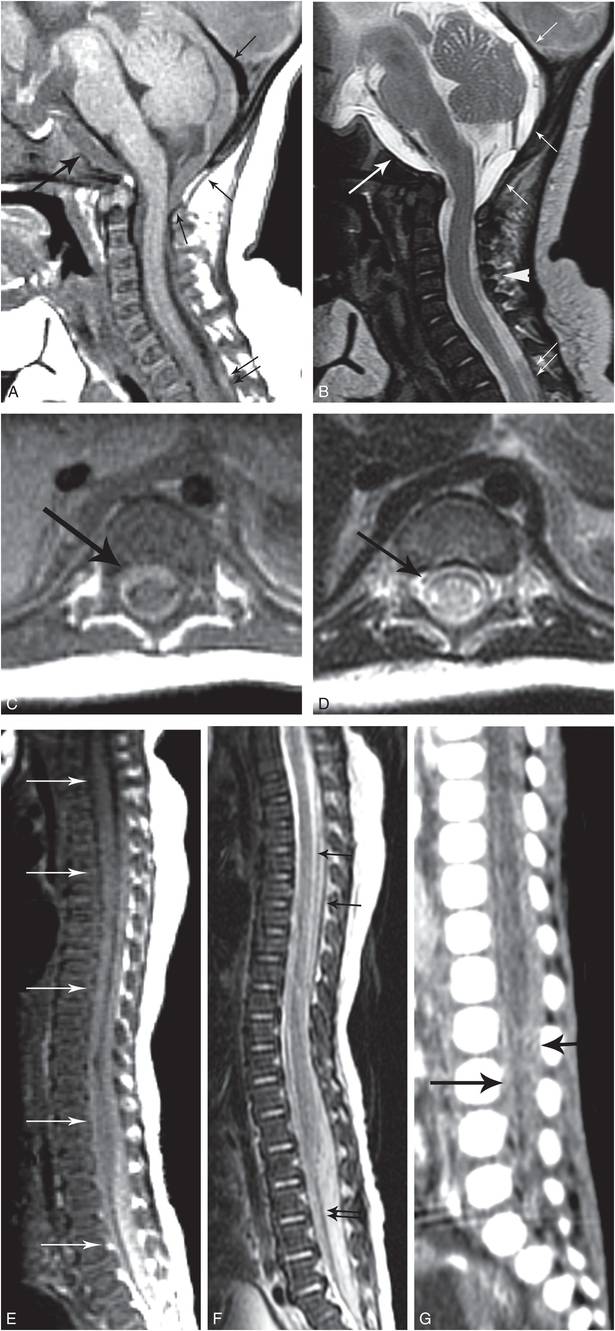
Figure 21.19 Spinal SDH. Five-month-old infant with lethargy and respiratory distress. (See same patient in Figs. 19.24, 22.25.) Additional imaging showed an occipital fracture, SDHs, HII, visceral injuries, and multiple fractures, including rib fractures and a CML. No RHs. A, Sagittal T1WI shows a subtle retroclival subdural collection (large arrow), an occipital SDH (small arrows), which extends through the foramen magnum into the cervical spinal canal, and a subtle posterior spinal SDH inferiorly (double arrows). B, Sagittal T2WI shows the retroclival subdural collection (large arrow), posterior occipital SDH (small arrows), and spinal SDH (double arrows), and edema of the interspinous ligaments (arrowhead). C, D, Axial T1W and T2W images show circumferential SDH (arrows) within the thoracic spine. E, F, Sagittal T1W and T2W images of the spine show spinal SDH extending from the cervical region to the distal thecal sac tip (arrows). Note the anterior displacement of the cauda equina (double black arrows in F). G, Sagittal reformatted image from the abdominal and pelvic CT demonstrates the hyperdense SDHs in the lumbar spinal canal (arrows).
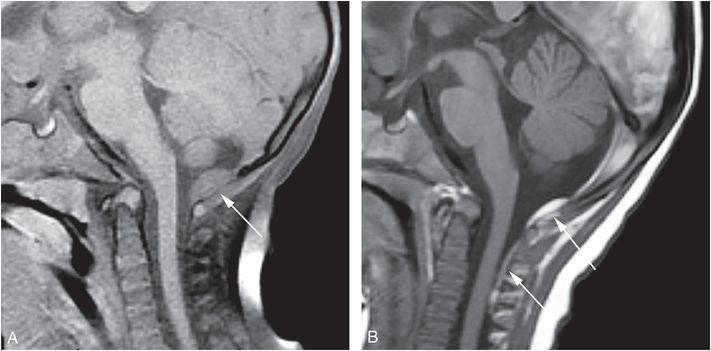
Figure 21.20 Spinal SDH on follow-up MRI. Seven-month-old who reportedly fell down a short set of stairs with the babysitter. The baby vomited, went limp, and developed seizures. There was an unexplained head bruise, retinoschisis and a negative SS. Brain imaging showed SDHs and HII. A, Sagittal T1WI image shows an intermediate signal intensity occipital SDH (arrow) and no subdural collection in the cervical region. B, Sagittal T1WI seven days later shows the posterior occipital SDH, which is smaller in size and brighter in signal intensity. A new SDH (arrows) is seen within the posterior aspect of the cervical spine, similar in signal intensity to the posterior fossa subdural collection, suggestive of distal run-off.
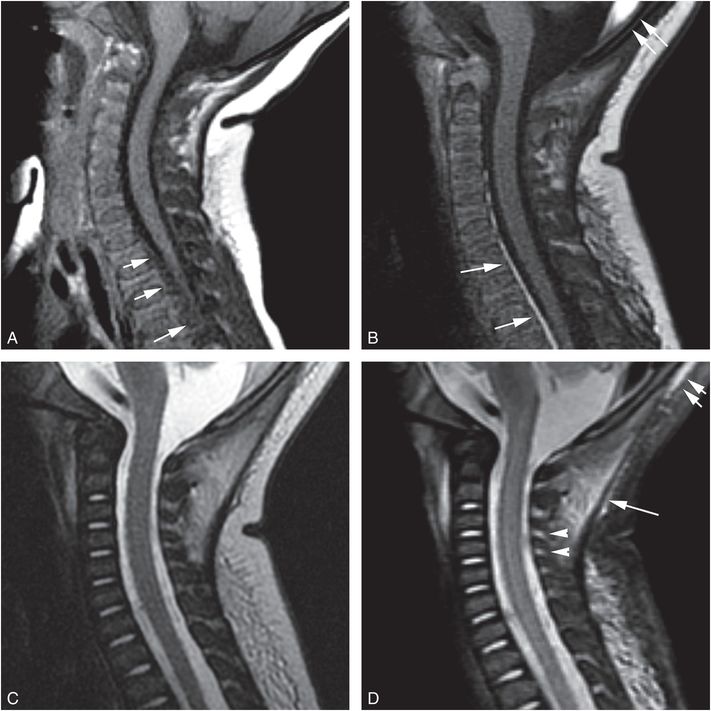
Figure 21.21 Spinal SDH. Three-month-old with increased irritability, lethargy, and a bulging fontanel. There was no history of trauma. Bilateral retinoschisis was noted. Imaging showed SDH, SAH, and HII. A, Sagittal T1WI FS on Day 1 shows a subtle spinal SDH (arrows), slightly hyperintense to CSF. B, Sagittal T1WI on Day 10 shows evolution of signal intensity of the SDH, which makes the collection more conspicuous (arrows). C, On the sagittal T2WI of the initial MRI, the SDH is not appreciable. D, Sagittal STIR image at presentation shows edema within the occipital scalp (double arrows), and deep cervical (single arrow) soft tissues and within the interspinous ligaments (arrowheads).
Some authors consider it unlikely that spinal SDHs arise from inferior tracking of supratentorial subdural blood, given anatomic barriers (e.g., the tentorium cerebelli) that exist between the supratentorial compartment and the posterior fossa (99). In the review by Koumellis et al. of 18 infants under 1 year of age with AHT and spinal MRIs, spinal SDHs were noted in 44% of children, all of whom had associated supratentorial and posterior fossa subdural collections (139). All spinal SDHs were similar in signal intensity to the subdural collections within the posterior fossa, but not to those within the supratentorial compartment, and two spinal subdural collections were in continuity with posterior fossa subdural collections across the foramen magnum. Most of the subdural collections were observed dependently in the thoracolumbar spine rather than within the cervical region. No child had imaging evidence of spinal cord injury, and all subdural collections were clinically occult. Two of 18 children had fractures of the thoracic spine identified on radiographs and one had an associated small EDH of the spine. In two patients the spinal SDHs were still present on the three-month follow-up MRI examination.
The largest review of spinal SDHs related to abuse was conducted by Choudhary et al. (138), whose findings were similar to those of Koumellis et al. (139). They studied 252 children under 2 years of age with AHT and spinal imaging, and compared those findings to that of a similarly aged cohort of children with accidental trauma. In the AHT cohort, 24 of 38 (63%) children with thoracolumbar spine imaging had a spinal SDH, compared to 1 of 70 (1%) children in the accidental group. Their results suggest that spinal SDHs occurring in the context of trauma may be relatively specific for an abusive mechanism. All children with spinal SDHs had concomitant supratentorial and posterior fossa SDHs of similar attenuation and/or signal intensity to that of the spinal SDHs. The authors also found the spinal SDHs to be predominantly asymptomatic and most were located within the thoracolumbar region, similar to the distribution noted by Koumellis et al. (139).
Spinal SDHs may be variable in size and extent and occasionally involve the entire spine (Fig. 21.19). In addition, a spinal SDH may not be evident on the first imaging study, but appears on a follow-up MRI examination, presumably as a result of distal run-off from a posterior fossa subdural collection (Fig. 21.20). Spinal subdural collections may be subtle in appearance and similar in signal intensity to CSF if blood products are hyperacute or if there is admixing of CSF with blood. A follow-up MRI may aid in the detection of SDHs as blood products evolve with time and become more conspicuous (Fig. 21.21). Spinal subdural collections are occasionally identified on CT (Fig. 21.19), although detection may be hampered by streak artifact across the spinal canal arising from bone. In addition, if the subdural collection is low in attenuation, it may be difficult to discern from the adjacent CSF. In Choudhary and associates’ study, spinal SDHs were identified on cervical spine CTs of children undergoing assessment for cervical spine injury and on abdominal and pelvic CTs of children being assessed for visceral injury (138). This underscores the utility of generating targeted reformatted images of the spine from the chest, abdomen, and pelvic CTs in sagittal and coronal planes with a small field of view to facilitate detection of these lesions (Fig. 21.19).
Sonography of the infant spine may also aid in detecting spinal subdural collections. Edelbauer et al. demonstrated spinal subdural effusions by sonography in six infants with AHT (150). The size of the collections was variable and some extended from the cervical spine to the cauda equina. Sonography is a useful alternative to MRI for detecting spinal SDHs in the unstable infant with AHT in the intenstive care unit setting in whom advanced spinal imaging cannot be performed.
Medullary and cervical spinal cord injuries
The incidence of spinal cord injury in the pediatric population ranges from under 1% to 10% of all spinal injuries (104). In most large series of pediatric cervical spinal cord injury, child abuse patients constitute only a small fraction of children studied or are not mentioned specifically (37, 96, 104, 151–156). Several series address spinal cord injury related to abuse, but the methodologic limitations of these studies do not permit reliable incidence estimates (14, 21, 131, 134, 144, 152).
The imaging literature that examines the relationship between abuse and medullary/cervical cord injury is sparse, as currently MRI of the cervical spine is not uniformly obtained in children with suspected AHT. When a cervical spine MRI is acquired, protocols and sequences may not be optimized for the size of a small child to permit identification of subtle cord injury. For example, if the imaging field of view is too large, subtle cord injury will be missed. Timing of imaging relative to injury is also important and if a cervical spine MRI is obtained in a delayed fashion, initial cord injury may no longer be evident. Additionally, diffusion-weighted imaging (DWI), an often helpful adjunct to routine sequences, may not be acquired (157).
Pathology and trauma-induced apnea
As with spinal trauma in general, the distribution of accidental spinal cord injuries is age dependent. Most spinal cord injuries in children involve the cervical cord (83, 158). In infants and young children, traumatic upper cervical cord injuries are more common and more severe than lower cervical cord injuries due to the inherent instability of the CCJ and upper cervical spine in younger patients (86, 98, 104, 159). Whereas spinal cord injuries in teenagers are most commonly accompanied by vertebral fractures with or without subluxation, younger children are more prone to cervical cord injuries with purely ligamentous damage (98, 104). It is reasonable to draw some inferences from these accident victims to spinal cord injuries occurring with abuse.
A number of pathology reports have identified lower brainstem and cervical cord/nerve root injuries in fatal cases of child abuse (132, 134, 144, 154, 160–162). The reported ability to detect such lesions at postmortem in children with abusive trauma varies widely, an observation that may be linked to differences in technique, as well as the proficiency and care of the examiner (161, 163). Postmortem imaging of cadavers with radiography, CT, and/or MRI may enhance the pathologist’s ability to detect significant findings (133, 145).
One of the most comprehensive forensic studies conducted on inflicted cervical spine injuries was performed by Brennan et al. (134). The authors evaluated fatal abusive injuries at postmortem examination in 52 children less than 2 years of age. Forty-one died of AHT and of these 29 (71%) had primary cervical cord injuries. The study findings were as follows: 21 of 29 (72%) had a cervical cord contusion, laceration, or transection; 16 of 29 (55%) had nerve root avulsions/dorsal root ganglion hemorrhages; 16 of 40 (40%) examined specimens in AHT cases had brainstem hemorrhage or laceration. Brainstem and spinal cord injury was not always present in children with cerebral HII, suggesting that although primary cervicomedullary injury is potentially an important factor in fatal AHT, it may not be the only cause (see below).
In contrast, Molina et al. reported a much lower incidence of neck injuries in a series of children less than five years of age who died from inflicted blunt force trauma (135). Eighty cases had head injury and only two children had trauma to the neck. Kasim et al. reported only 1 case of cervical cord injury in a series of 30 children with fatal inflicted trauma (164). Three additional forensic reports describe inflicted cervical cord injury: Hart et al. described a young child with head injury and spinal cord hemorrhage (145); Rutty et al. reported two young children with AHT and cervical nerve root damage (129); and Miziara and Bertaccini described the autopsy findings in a young child with hyperextension injury of the CCJ, as well as brainstem hemorrhage and edema (165).
In recent years, attention has been directed toward cervical spinal cord and medullary injuries in an effort to understand the mechanisms responsible for the clinical entity known as the shaken baby syndrome (SBS). There is growing evidence to support the view that injuries involving the CCJ are associated with apnea and HII in some abused infants (132, 144, 160, 161). As inflicted cervical spine trauma is often associated with AHT and commonly results in significant and permanent neurologic alterations, these relatively uncommon injuries are deserving of in-depth discussion (9, 11, 14, 17, 20–23, 26, 30, 31, 34, 36, 37, 67, 73, 110, 111).
Efforts to understand the role of brainstem and upper cervical cord injury in cases of AHT stem from the known association between damage to these regions and respiratory compromise in cases of accidental trauma. Bohn et al. examined 19 children with severe accidental traumatic brain injury (TBI) and absent vital signs or severe hypotension at presentation, which could not be explained by blood loss or airway obstruction (163). Cervical cord lacerations or cervical cord hemorrhage were found in 16 cases at autopsy and 14 children had CCJ injury detected by imaging. Based on these findings, the authors concluded that children with severe head trauma most commonly injure the high cervical spine, which in turn causes immediate damage to the cervical cord, inducing apnea and cardiac arrest. Meyer et al. came to similar conclusions in a study of children with accidental high cervical spine injury presenting with apnea or cardiorespiratory arrest (166). All children had severe head trauma and grossly visible brainstem contusions on CT, or imaging findings that were suspicious for such injuries. The authors concluded that in young comatose children with severe distracting injuries of the upper cervical spine, CCJ injury and brainstem lesions should be suspected.
Reports of medullary and high cervical spine injury in fatal cases of AHT are sparse in the early child abuse literature. In 1984, Calder et al. were among the first to report such an injury in a 2-year-old boy with AHT and a brainstem lesion (167). The authors provided no further details. In 1989, Hadley et al. drew attention to spinal cord injury in cases of abuse in a series of severely abused young children, including 6 cases that were autopsied (131). Of these, four had high ventral cervical cord contusions and all had marked brain swelling and herniation. The diagnoses of cervical cord contusion were made on the basis of gross examination of the cord at autopsy.
In 1995, Johnson et al. examined the relationship between cerebral HII in young children with AHT and apnea (144). In this series, all children had AHT and most had significant signs of respiratory distress and hypotension. Four children underwent autopsy; in one infant the cervicomedullary junction was not examined, but in the other three infants injury of the cervicomedullary junction was found. The authors concluded that brainstem and cervical cord injury are the likely cause of apnea and that trauma-induced apnea, in turn, causes cerebral HII in children with AHT.
Others have similarly invoked brainstem injury as a causative mechanism for HIE in abused children. In 1998 Shannon et al. studied the cervicomedullary junction in children with fatal AHT and showed histologic evidence of axonal damage of the medulla and cervical cord based on immunohistochemical staining and expression of beta-amyloid precursor protein (162). Beta-amyloid precursor protein is considered a sensitive marker for axonal damage (168, 169), but it is not specific for traumatic axonal injury. In this study, investigators examined 14 young children with severe neurologic deficits and AHT. Of these children, all had evidence of cerebral edema, 10 had injury of the medulla, and 7 had injury of the cervical spinal cord and spinal nerve roots with a predilection for the glial head.
Geddes et al. also demonstrated axonal injury of the cervicomedullary junction in victims with fatal AHT (132, 160). They examined the brains of 53 children less than 8 years of age. Focal axonal injury of the brainstem involving the corticospinal tracts in the caudal pons and medulla was noted in eight infants, and in three infants, axonal damage of the cervical cord roots was also detected. The authors proposed that injury to the cervicomedullary junction had occurred secondary to stretch from cervical hyperextension/flexion, and that infants with severe AHT may die as a consequence of respiratory failure rather than from direct TBI.
Oehmichen et al. challenged this hypothesis of primary injury to the respiratory centers as the cause of respiratory compromise and HII in abused children (133). They examined 18 infants with fatal AHT and found that only 2 of 13 (16%) infants had axonal injury of the CCJ, and only 1 (8%) had axonal injury of the nerve roots of the CCJ. The authors concluded that axonal injury is not generally observed in the medulla, cervical spinal cord, or nerve roots in children with AHT.
Matshes et al. focused on the relationship between hyperextension and flexion injuries of the neck and cervical nerve root trauma (161). The authors examined a series of young children who sustained hyperflexion/extension forces to the neck and compared these children to controls who died of other disease-related causes. All of the hyperflexion/extension cases had either unilateral or bilateral intraneural or perineural hemorrhage of the roots of C3–5, with injury to the C2, C6, and C7 nerve roots less commonly observed. Only one of the control cases had signs of nerve root damage and this child died under circumstances that were concerning for abuse. Many of the children with nerve root injuries also had anoxic brain injury. Based on these results, the authors proposed that injury to cervical nerve roots may result in disrupted innervation to the diaphragm, which in turn causes respiratory compromise, apnea, and secondary anoxic brain injury.
In an important recent study, Kadom et al. explored the relationship of cervical injuries with intracranial pathology in cases of abuse and children with accidental injuries (37). The authors conducted a 3-year retrospective review of children less than 36 months of age evaluated for head trauma between 2008 and 2010. The study included 74 children (mean age: 164 days; range: 20–679 days). There were 26 children with AccT and 38 with AHT (N = 18 presumptive AHT, N = 20 suspicious for AHT), and 10 with undefined head trauma. Cervical spine injuries were found in 27 of 74 (36%) children, mostly ligamentous in nature. One child had intrathecal spinal blood and two had spinal cord edema; all three of these children had ligamentous injury. Cervical injury did not show a significant relationship with AHT or permit discrimination between accidental and AHT. Notably, of the 30 children with supratentorial brain injury, 16 (53%) had a bilateral hypoxic ischemic pattern. There was a statistically significant relationship between bilateral cerebral HII and AHT (P <0.05). Importantly, 81% of children with bilateral HII brain injuries had cervical injuries. The authors concluded that although detection of cervical spine injuries by MRI does not discriminate between accidental and AHT, it can help to distinguish a traumatic from nontraumatic ICI. Their data, as well as the 2014 study of Choudhary et al., lend strong support to the hypothesis of a causal relationship between cervical injuries and cerebral HII in cases of AHT (37, 66).
Mechanism of injury
Mechanisms of injury proposed for traumatic cervical cord injury include cervical hyperextension, hyperflexion, stretch/distraction, and ischemia (98, 105). In a child with inflicted cord injury, one or more of these mechanisms may be at work. For instance, Gleckman et al. reported postmortem findings in a two-month-old abused child with AHT and a cervical cord infarct and found narrowing of the vertebral artery caused by periadventitial hemorrhage (170). Systemic hypotension, which is commonly present in severely abused children, may also contribute to cord ischemia or infarct secondary to low arterial perfusion pressure and impaired autoregulation of blood flow (96).
Many investigators believe that shaking/whiplash events account for the intracranial injuries commonly observed in children with AHT (171–173), and it may be inferred that in some cases, infant necks are injured in a similar manner. Others have suggested that inflicted cervical cord injury may be sustained by holding a child by the head or neck while swinging the body. In support of this mechanism of abuse, Piatt and Steinberg described a child with inflicted cervical spine injury and ecchymosis below the jaw (14). Parrish reported a case of isolated spinal cord injury in a two-month-old infant with compression injuries of the eyes (174). He theorized that the perpetrator had grasped the child’s head by positioning his thumbs over the eyes, while shaking the child’s body. Similarly, Case described two siblings with cervical cord injuries: in one child the father described shaking the child by grasping the head; the other child had hematomyelia of the upper cervical cord and medulla with petechial hemorrhages over the bulbar conjunctiva, suggesting a similar mechanism of injury (175). Lastly, Feldman et al. noted the absence of retinal hemorrhages in a series of abused children with cervical cord injuries, suggesting that a mechanism other than shaking may have been responsible for the spinal injuries (21).
Clinical issues
Cervical cord injury can be clinically evident or occult, in which case the diagnosis may be delayed or missed (14, 58, 82). It can be overlooked in children: (1) with concurrent brain trauma; (2) on mechanical ventilation; and (3) with a delayed onset of spinal cord symptomology (98).
Although most reported spinal cord injuries are accompanied by spine fractures or gross spinal instability, there are reports of isolated spinal cord injuries without bony involvement (14, 18, 21, 35, 44, 176). Occult spinal cord injury, referred to as spinal cord injury without radiographic abnormality (SCIWORA), accounts for 4–67% of all pediatric spinal trauma and is a major concern in the clinical evaluation of traumatized children (98, 177, 178). The acronym SCIWORA was first coined in 1982 by Pang and Wilberger, who described acute traumatic myelopathy in children with normal radiographic, myelographic, tomographic, and CT studies (96). SCIWORA most often occurs in children, particularly in those under the age of three years (86, 96, 159). It is hypothesized to occur in cases of traumatic deformation of the spine causing transient intersegmental displacements followed by rapid recoil and self-reduction of the vertebral column, resulting in spinal cord injury without residual spinal misalignment (98). The mismatch between the deformability of the developing spine and the spinal cord causes injury to the cord in the absence of bony pathology. Prior to MRI, children with nonosseous traumatic lesions were routinely diagnosed with SCIWORA. However, since the introduction of MRI in the early 1990s, patients with symptomatic spinal cord injury and negative neuroimaging are much less common.
Imaging
Despite the number of forensic reports on inflicted spinal cord injury, there are relatively few imaging studies that examine these lesions in relation to abuse. Kemp et al. found only eight well-documented abusive cervical cord injuries in living children in their review of the literature (74). Swischuk was one of the first authors to draw attention to spinal cord injuries in child abuse (18). He described a two-year-old girl with marked prevertebral soft tissue swelling and significant cervical cord enlargement on myelography, which represented either cervical cord edema or intramedullary hemorrhage. In a series of 58 children with acute traumatic spinal cord injury reported by Kewalramani et al. investigators identified 1 child with inflicted spinal cord injury for whom no further details were provided (152).
In the series of 25 children with SCIWORA by Pang and Wilberger, 1 case of child abuse was noted – a 1½-year-old child with AHT and cervical cord injury manifested as partial C5 myelopathy (96). Osenbach and Menezes reported a series of 31 children with SCIWORA that included 1 case of child abuse – a 22-month-old child with spinal cord injury (86). In a review of 23 cases of child abuse and central nervous system involvement, Benzel and Hadden found 1 case with cervical cord injury – a 9-week-old boy with inflicted trauma who “quit moving his arms” (179). Myelography demonstrated swelling of the cervical cord, and no bony abnormality of the cervical spine. Grabb and Pang reported a series of 18 children with SCIWORA (the classic definition of SCIWORA was applied in this study, excluding MRI data) that included one case of child abuse – a 21-month-old child with complete C3 cord syndrome and MRI findings of cervical cord edema and hemorrhage extending from C3 to T1 (44). The follow-up MRI showed complete cord atrophy from C3 to C7.
Feldman and others reported the imaging findings of five abused children with cervical cord injury identified by MRI: three children had medullary hemorrhage, cord edema, and cord hemorrhage; one child had cervical cord edema and hemorrhage; and one child had a cervical cord transection (Fig. 21.22) (14, 20, 21). Rooks et al. described the imaging findings in 3-month-old twin girls who had been abused: one had a C5 fracture and a C4–5 dislocation; and the other had a C5 fracture with a C5–6 dislocation (see Figs. 21.16, 21.17) (17). Both infants had associated cervical cord compression and neither child had ICI by MRI.
Figure 21.22 Brainstem and cervical cord injury. Six-month-old with lethargy and respiratory distress, who subsequently developed central cord syndrome. Brain imaging showed a skull fracture without parenchymal injury. There was no cervical fracture, but SS revealed multiple fractures in other regions. Shaking was confessed. Sagittal T2WI shows edema and hemorrhage in the cervical cord (1) and medulla (2). (With permission from Feldman KW, Avellino AM, Sugar NF, Ellenbogen RG. Cervical spinal cord injury in abused children. Pediatr Emerg Care. 2008;24:222–7.)
Related posts:
 Abusive head trauma: intracranial imaging strategies
Abusive head trauma: intracranial imaging strategies
 The physics and biology of magnetic resonance imaging: medical miracle anyone?
The physics and biology of magnetic resonance imaging: medical miracle anyone?
 Differential diagnosis V: obstetric trauma
Differential diagnosis V: obstetric trauma
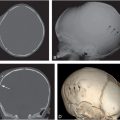 Abusive head trauma: scalp, subscalp, and cranium
Abusive head trauma: scalp, subscalp, and cranium
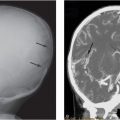 Abusive head trauma: extra-axial hemorrhage and nonhemic collections
Abusive head trauma: extra-axial hemorrhage and nonhemic collections
 Bony thoracic trauma
Bony thoracic trauma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


