After studying this chapter, the student will be able to:
1. Explain the reasons for nasogastric and nasoenteric intubation and the technologist’s responsibilities when these tubes are in place.
2. Describe the precautions needed when caring for a patient who has a gastrostomy tube in place.
3. Describe the patient care considerations when working with a patient who requires parenteral nutrition or has a central venous catheter.
4. Describe the symptoms of a patient who needs suctioning and explain the action the technologist would take in this situation.
5. Explain the precautions necessary when working with a patient who has a tracheostomy.
6. List the precautions that are required when working with a patient requiring mechanical ventilation.
7. List the patient care precautions taken for the patient who has a chest tube in place with water-sealed drainage.
8. Describe the patient care considerations for the patient who has a tissue drain in place.
KEY TERMS
Asphyxiation: Severe hypoxia leading to hypoxemia, hypercapnia, loss of consciousness, and death
Bolus: A concentrated mass of a pharmaceutical preparation, such as an opaque contrast medium given intravenously or swallowed
Cannula: A tube used to allow fluids, gases, or other substances into or out of the body
Dyspneic: Having shortness of breath or difficulty breathing
Fowler position: Position in which the head of the patient’s bed is raised 18 to 20 inches above the level of the heart with the knees also elevated
Gastrostomy: Creation of an opening in the stomach to provide food and liquid administration
Hemostat: A clamp-like instrument used to control flow of fluids or blood
Lavage: The process of washing out an organ, usually the stomach, bladder, or bowel
Nasoenteric tube: A tube made of the same materials and inserted in much the same way as a nasogastric tube; however, a nasoenteric tube is allowed to pass into the duodenum and small intestine by means of peristalsis
Nasogastric tube: A tube of soft rubber or plastic inserted through the nostril and into the stomach
Saline solution: A solution consisting of a percentage of sodium chloride and distilled water that has the same osmolarity as that of body fluids
Nasogastric (NG) and nasoenteric (NE) tubes are inserted for therapeutic and diagnostic purposes. These tubes have a hollow lumen through which secretions and air may be evacuated or through which medications, nourishment, or diagnostic contrast agents may be instilled. The radiographer must be able to care for and transport patients with these tubes in place. The purposes of gastric suction and the ability to attach or discontinue it when the physician’s orders require it must also be understood to prevent any injury to the patient.
Abdominal images may be required before, during, or after the passage of NG or NE tubes. This image can be performed either in diagnostic imaging department or with a mobile x-ray machine bedside. Although radiographers do not insert these tubes, preparation of the patient may be required if the tube is to be inserted in the diagnostic imaging department. What type of equipment to assemble and how to assist with the procedure are requisite knowledge.
Occasionally, a patient requiring a procedure will have a gastrostomy tube in place. These tubes may be required for persons who are gravely debilitated and unable to obtain nutrition in a normal physiologic manner. These patients must be cared for in a safe and sensitive manner.
Patients who are unable to take in nutrients though the gastrointestinal (GI) system, either partially or completely, may be nourished intravenously. This can be accomplished in the short term parenterally by peripheral intravenous means and in the long term by reliance on central venous catheters.
Occasionally, it is necessary for the patient who has vomited or who has an accumulation of blood or secretions in the mouth or throat to be suctioned while under the care of the technologist. Although the technologist does not perform these procedures, a quick assessment of the patient is critical so that the procedure can be done quickly to prevent aspiration of the fluid into the lungs or cause respiratory failure.
Patients with the tracheostomy tubes in place may also need diagnostic imaging examinations. They must receive proper care to prevent injury and to keep them comfortable while the examination is in progress.
Patients who are unable to maintain adequate respiration may require mechanical ventilation to support life. Mobile chest imaging examination for these patients is a frequent occurrence; therefore, precautions when working with patients on a ventilator are required.
Chest tubes are inserted after surgical procedures, injury, or diseases of the lungs to permit drainage of fluid or air out of the pleural space. If air and fluid become trapped in the pleural space, pressure builds and creates what is called a tension pneumothorax. If this condition is not relieved, the resulting respiratory distress may produce a life-threatening situation. The precautions needed to care for patients with a chest tube must also be learned.
After surgical procedures, a variety of tissue drains are placed in the areas of the body that cannot tolerate an accumulation of fluid. The radiographer must be able to recognize these drains and direct patient care in a manner that prevents dislodging the drains during the imaging process.
NG AND NE TUBES
NG tubes are made of polyurethane, silicone, or rubber. They are inserted through the nasopharynx into the stomach, the duodenum, or the jejunum. If a patient has an anatomic or physiologic reason why the nose cannot be used for passage, the tube may be inserted through the mouth over the tongue. NG tubes are also used for diagnostic examinations, for administration of feedings or medications, to treat intestinal obstruction, and to control bleeding (Table 13-1).
CALL OUT
The technologist is often asked to perform a mobile abdomen x-ray for NG tube placement at the patient’s bedside.
NE tubes are made of the same materials as NG tubes and are inserted in much the same way as NG tubes; however, they are allowed to pass into the duodenum and small intestine by means of peristalsis. They are also used for decompression, diagnosis, and treatment purposes (Table 13-2).
Two of the most common NG tubes are the Levin and the sump tube (Fig. 13-1). Other NG tubes often seen are the Nutriflex, the Moss, and the Sengstaken-Blakemore (S-B) esophageal NG tube. The Levin tube is a single-lumen tube with holes near its tip. The sump tube is a radiopaque, double-lumen tube. The opening of the second lumen is a blue extension off the proximal end of the tube. This is the end that remains outside and is called a “pigtail.” This end is always left open to room air for the purpose of maintaining a continuous flow of atmospheric air into the stomach, thereby controlling the amount of suction pressure that may be placed on the gastric mucosa. This is a means of preventing injury and ulceration of these tissues.
The Nutriflex tube is used primarily for feeding. It has a mercury-weighted tip and is coated with a lubricant that becomes activated when moistened by gastric secretions.
The Moss tube is a more complex triple-lumen tube. One lumen has an inflatable balloon to anchor it in the stomach. The second lumen is used for aspiration of fluid, and the third is for duodenal feeding (Fig. 13-2).
The S-B tube is also a triple-lumen tube; two of the lumens have balloons. The balloons are inflated to exert pressure on bleeding esophageal varices. The third lumen is used for lavage and to monitor for hemorrhage. The balloon pressure must be maintained at all times, but if the patient becomes dyspneic, the balloon pressure must be relieved at once by cutting the balloon lumens with scissors. If the patient will be in the imaging department for a lengthy period, the technologist should not attempt to care for a patient with an S-B tube in place without the patient’s nurse on hand. Asphyxiation or aspiration of gastric contents into the lungs is possible without keen and continuous monitoring. The patient with an S-B tube in place is usually cared for in the intensive care unit (ICU), and portable images are ordered.
TABLE 13-1 Common Nasogastric Tubes
Name
Number of Lumens
Description
Use
Levin
1
Plastic tube that is passed through the nose into the stomach
Gastric decompression
Sump
2
Radiopaque tube with a plug pigtail that lets airflow into the stomach
Drain fluid from the stomach
Nutriflex
1
Mercury-weighted tip; coated with a gastric secretion-activated lubricant
Feedings
Moss
3
Has a balloon to anchor into the stomach, whereas the second and third lumens are used for aspiration and feeding
Aspiration of fluid; duodenal feeding
Sengstaken-Blakemore
3
Thick catheter with two balloons used to exert pressure against the walls of the esophagus
Control of bleeding from esophageal varices
Three of the most commonly used NE tubes are the Cantor, the Harris, and the Miller-Abbott. The Cantor and Harris tubes have a single lumen, whereas the Miller-Abbott tube is a double-lumen tube. One lumen of the Miller-Abbott tube is used for intestinal decompression, and the other is for the introduction of mercury after insertion. Some single-lumen tubes are weighted with a metal tip. The progress of the tube may be observed in the diagnostic imaging department fluoroscopically. Radiographs are taken after passage of these tubes to establish correct placement (Fig. 13-3).
TABLE 13-2 Common Nasoenteric Tubes
Name
Number of Lumens
Description
Use
Cantor
1
Long tube with a small mercury-filled bag at the end; contains drainage holes for aspiration
Relieves obstructions in the small intestine
Harris
1
Mercury-weighted tube passed through the nose and carried through the digestive tract by gravity
Gastric and intestinal decompression
Miller-Abbott
2
Long small-caliber catheter; one is a perforated metal tip, and the other has a collapsible balloon; radiopaque tube
Decompression
Passage of NG and NE Tubes
Technologists are not responsible for inserting NG or NE tubes. A registered nurse usually inserts an NG or NE tube, or a physician may insert the NE tube. Insertion of a tube is an uncomfortable and frightening procedure for the patient, who is often very ill. If this procedure is to take place in the imaging department, explain to the patient what is being done and for what purpose. Ensure the patient that if he or she concentrates on swallowing and breathing as the tube is inserted, the procedure will go smoothly and quickly.
The physician may swab the nasal passages and spray the oropharynx with tetracaine (Pontocaine) to promote the patient’s comfort by anesthetizing the area and suppressing the gag reflex. A gargle with a liquid anesthetic may also facilitate the procedure.
The patient is placed in a Fowler position with pillows supporting the head and shoulders. When the physician or nurse is ready to insert the tube, the distal end is lubricated with a water-soluble lubricant, and the patient is instructed to swallow as it is passed. The tube should go down easily and with little force. When the tube is believed to be in the stomach, as shown in Figure 13-4, an initial radiographic image verifies its position. If the tube is to be in place for a considerable length of time, its placement may be verified by attaching the end of the NG tube to a 20- to 30-mL syringe and withdrawing gastric fluid. The fluid is tested with litmus paper, which must test acidic to ensure that the tube is in the correct position. When it is certain that the tube has reached the stomach, reassure the patient and make him or her comfortable. NG tubes are taped in place, but NE tubes are not taped because their position is achieved through peristaltic action. The Levin tube is securely taped so that it is not accidentally withdrawn. It should never be necessary to repeat passage of a gastric tube because of careless handling. There should be no pulling pressure on the tube. Patients with gastric tubes in place are not to eat or drink anything unless the physician specifically orders it. Patients who may accidentally pull their NG tubes out may have immobilizers on their wrists.
FIGURE 13-2 The Moss esophageal duodenal decompression and feeding tube has three chambers; the first anchors it in the stomach, the second is for aspiration, and the third is for feeding.
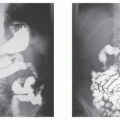
FIGURE 13-3 (A) Radiograph of a small bowel obstruction with a NE tube in place. (B) Radiograph of a small bowel ileus with a NG tube in place.
The placement of an NG tube must be ascertained before any medication, food, water, or contrast agent is administered into it. If this is not done, accidental administration of an agent into the pleural cavity may occur with adverse consequences for the patient.
The correct position of an NG or NE tube initially may be determined with a radiographic image or by fluoroscopy. Obviously, a radiographic image cannot be used each time it is necessary to know whether the tube is correctly positioned. The other means of determining the correct placement of an NG or NE tube is by aspirating the contents of the stomach or the bowel through the tube with a syringe. The aspirant is then tested with litmus paper to measure its acidity. Gastric contents are acidic (approximately pH 3). The pH of intestinal secretions is less acidic (approximately 6 to 6.5). The pH of respiratory secretions is not acidic (7 or greater). Note that pH levels of small bowel and respiratory secretion are similar but are far greater than intestinal secretions. Tubes properly placed in the stomach show a pH in the range from 1 to 4.
If there is any doubt concerning the position of an NG or NE tube, nothing should be administered into it. If instillation of an agent has begun, discontinue it immediately. If the patient seems to have regurgitated gastric contents, the technologist must summon assistance immediately and prepare to assist with suctioning. To reduce the risk of aspiration, the patient with an NG or NE tube should be placed in a semi-Fowler position during and for 30 minutes after administration of any medium into the tube.
FIGURE 13-4 Radiograph taken after insertion of an NG tube, to verify the tube’s position.
CALL OUT
A small bowel series examination may be ordered for patients with an NG tube by their physician. The contrast media is instilled via the NG tube according to department protocols.
NE Feeding Tubes
These are several narrow-lumen tubes that are inserted for the purpose of feeding patients. They are used for patients who are unable to obtain nourishment or take oral medications in a natural manner and who are expected to obtain nourishment by this method for some time. Various forms of nutritional supplements may be prescribed depending on the patient’s needs. The feedings may be given by continuous gravity drip, by bolus, or by a controlled pump method. Patients may be discharged from the hospital with these tubes in place.
Removing Gastric Tubes
The Levin tube, the sump tube, and other tubes positioned in the stomach are easily removed; however, it must never be assumed that simply because an imaging examination that involved its use is complete, it is permissible to remove the tube. Unless ordered by the physician to remove the tube, it must be left in place.
Do not remove NE tubes. The physician or registered nurse may remove the tube, or it may be passed through the intestinal tract and removed rectally. Although it is not in the purview of the technologist to remove the NG tube, Table 13-3 identifies the equipment that will be necessary to have on hand and describes the procedure in the event the radiographer is required to assist in the procedure.
CALL OUT
Radiographers are never to remove an NE tube.
Transferring Patients with NG Suction
NG and NE tubes are used before or after surgical procedures that involve the digestive system, for illness of the GI system to keep the stomach and bowel free of gastric contents, and for gastric decompression. The tube may be attached to a suction apparatus that is either portable or piped into the room from a central hospital unit (Fig. 13-5). The suction is maintained either continuously or intermittently, as the patient’s needs demand. When the technologist is responsible for transferring a patient who is having either continuous or intermittent gastric suctioning, the physicians’ orders must be verified before making the transfer. If it is permissible to discontinue the suction, the length of time that it can be interrupted safely must be known. If it is for only a short time, be certain that suction can be reestablished in the diagnostic imaging department. This can be accomplished by taking the patient’s portable suction machine with him or her or by using the suction available in the department. The amount of suction must also be known so that the pressure can be accurately adjusted. The amount of pressure that is ordered varies, and the correct level can be determined by reading the physician’s orders or by asking the nurse in charge of the patient to do this. The maximum amount of suction that can be used is a pressure equal to 25 mm Hg for an adult patient. More than this can damage the gastric mucosa.
Only gold members can continue reading. Log In or Register to continue