Abstract
FDG-avid adrenal lesions may be malignant (metastases, lymphoma, adrenal cortical carcinoma) or benign (such as adenomas). Most benign adrenal neoplasms demonstrate background FDG avidity; however, a small percentage of adenomas and other benign neoplasms are FDG avid and need to be distinguished from malignancy. Characteristic CT and MR findings of lipid-rich adenomas are diagnostic of a benign lesion, despite FDG avidity.
Keywords
FDG, PET/CT, adrenal, metastases, adrenal cortical carcinoma, adenoma, myelolipoma
The differential diagnosis for adrenal lesions includes malignant neoplasms, benign neoplasms, and benign nonneoplastic processes. The most common adrenal malignancies by far are metastases. Additional adrenal malignancies include lymphoma, malignant pheochromocytomas, and adrenal cortical carcinomas. The most common benign adrenal neoplasms are adenomas. Additional benign adrenal neoplasms include myelolipomas, benign pheochromocytomas, and ganglioneuromas. Nonneoplastic processes that involve the adrenal gland may include physiologic adrenal fluorodeoxyglucose (FDG) avidity, adrenal hyperplasia, infections, and traumatic lesions.
Adrenal Metastases
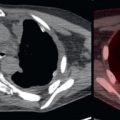
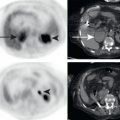
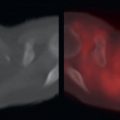
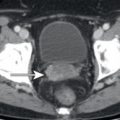
The adrenal glands are a common site of metastases. The most common primary tumors causing adrenal metastases are pulmonary, gastric, and esophageal malignancies; however, a very wide range of primary malignancies may result in adrenal metastases. Adrenal metastases are usually FDG avid and are associated with corresponding adrenal masses on computed tomography (CT) ( Fig. 15.1 ). In patients with primary malignancies with known propensity to metastasize to the adrenal glands, FDG-avid adrenal masses are suspicious for metastases until proven otherwise. FDG avidity on FDG positron emission tomography (PET) may help to highlight small adrenal metastases that could be overlooked on CT ( Fig. 15.2 ). Although less common, early adrenal metastases or adrenal metastases from malignancies that are not highly FDG avid may not demonstrate appreciable FDG avidity. Occasionally, non–FDG-avid adrenal metastases may need to be detected on the corresponding CT images ( Fig. 15.3 ).



Adrenal Lymphoma
Similar to lymphoma of other organ systems, lymphoma involving the adrenal glands is often FDG avid. Adrenal lymphoma may be primary or secondary. The majority of adrenal lymphomas are due to secondary involvement, whereas primary adrenal lymphoma is rare ( Fig. 15.4 ). After diagnosis, FDG PET provides valuable information about response to therapy in hepatic lymphoma, similar to other sites of lymphomatous involvement. Reduction of FDG avidity to less than liver background is considered treated lymphoma, whereas residual FDG avidity greater than liver background is suspicious for residual active lymphoma.

Adrenocortical Carcinoma
Adrenocortical carcinomas (ACCs) are rare and highly aggressive malignancies with poor prognosis. On CT or magnetic resonance (MR), ACCs are typically large heterogeneous suprarenal masses. Data on FDG avidity of ACCs are limited; however, ACC is usually FDG avid ( Fig. 15.5 ). Hemorrhage, necrosis, and calcifications are common. Areas of necrosis may not be appreciably FDG avid. ACC is known for rapid growth and invasion of adjacent organs and adjacent veins, such as the renal vein and inferior vena cava. Extension into the renal vein and inferior vena cava may be FDG avid.