Chapter 13 Alternative methods of intrapartum fetal surveillance
Despite the limited contribution of birth asphyxia to cerebral palsy and doubts cast on the benefits of intrapartum electronic fetal monitoring, research is in progress to find better methods of monitoring to avoid the tragedies which can occur due to birth asphyxia. Every now and then such tragedies are highlighted by litigation and the large awards of damages. There is little doubt that the practice of intrapartum fetal monitoring is likely to stay, but whether it will be in the form of electronic fetal heart rate (FHR) monitoring or by other means, or a by a combination, is difficult to predict. This chapter reviews why there is a search for newer methods, some of the newer methods available and what may happen in the future.
WHY IS THERE A SEARCH FOR NEW METHODS?
There are problems in correlating FHR changes with fetal acidosis. When all four features of the cardiotocograph (CTG) trace are normal, the chances of fetal acidosis are small. When all the features are abnormal just over 50% are noted to be acidotic.113 Depending on the physiological reserve of each fetus, one may respond differently from another to the hypoxic insult. It has been observed that for 50% of appropriately grown term fetuses with clear amniotic fluid to get acidotic, it takes 115 min with repetitive late decelerations, 145 min with repetitive variable decelerations and 185 min with a ‘flat trace’ (i.e. with reduced baseline variability).15 This implies that some appropriately grown term fetuses may become acidotic in a shorter period. This duration may be even shorter when there is reduced physiological reserve, i.e. in cases with infection, bleeding, post-term, growth-restriction and in those with scanty, thick, meconium-stained fluid. Therefore, it becomes necessary to determine the fetal condition when there are abnormal FHR changes by fetal scalp blood sampling (FBS). This will help to identify those in need of delivery and to avoid unnecessary operative intervention. However, the facilities and expertise are not available to perform FBS in many centres,136, 137 and its value is questioned by some.131 It is also known that FBS is done when it is not warranted and is not done when it is needed.138 In addition, the intermittent nature of the readings also makes it difficult to identify the optimal time to intervene without compromising the fetus, without increasing operative interventions. These issues have prompted research into newer methods of fetal surveillance in labour which are used as adjuncts to CTG in some centres.
FETAL ELECTROCARDIOGRAPH WAVEFORM ANALYSIS
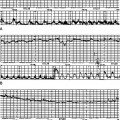
Experimental data have suggested that the appearance of high-peaked T waves together with an elevation of the ST segment signifies an imbalance of the myocardial energy situation with anaerobic metabolism and myocardial glycogenolysis. This important defence mechanism is known to operate with an increase in circulating catecholamine (β-adrenoceptor stimulation):139 this brings about a shift in K+ which increases the T-wave amplitude (T/QRS ratio) (Fig. 13.1A and B). The detection of ST changes are computerized and the STAN equipment highlights any significant changes in the ST segment. The ST events detected may be a baseline rise of the T/QRS ratio, an episodic rise of the T/QRS ratio or a biphasic ST segment. Each fetus has a steady level of T/QRS ratio in early labour that could be identified from the initial recording. The rise in the T/QRS ratio is calculated in reference to the lowest T/QRS ratio calculated over a period of 20 min in the previous 3 h period. This means that the equipment needs to be used for 20 min to calculate the baseline T/QRS ratio prior to major changes in heart rate or the ECG. In the immediate 20 min after start up, and when there are poor discontinuous signals, manual data analysis is required. A preterminal trace that shows total lack of baseline variability and reactivity, with or without decelerations, and a prolonged deceleration warrant immediate delivery.
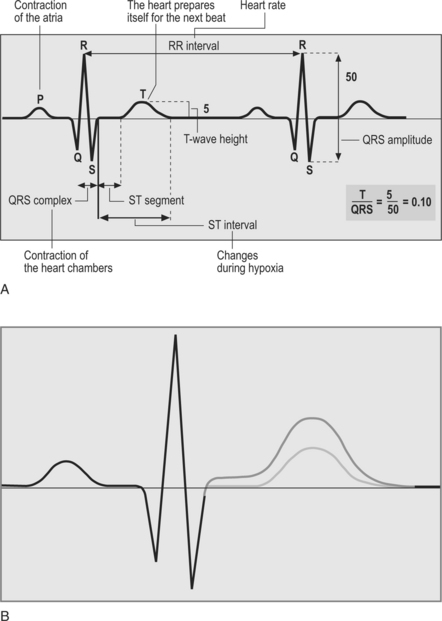
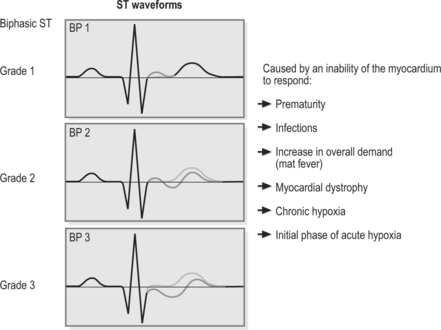
A steadily increasing T/QRS rise is termed a baseline rise, and if the ratio increases significantly and comes down within a brief period of a few minutes it is termed an episodic rise. The biphasic event refers to alteration of the ST segment where there is an initial rise and then a fall (Fig. 13.2). If the ST change is above the isoelectric line, it is termed biphasic 1; if it cuts the isoelectric line it is called biphasic 2; and if it is below the isoelectric line it is called biphasic 3. Biphasic 2 and 3 are considered significant and are related to the electrical flow from endocardium to epicardium. Hence these changes may present themselves in the following situations: when the myocardium is thin (e.g. preterm fetuses), there is myocardial disease, infection and hypoxia.140
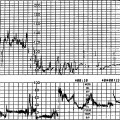
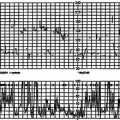
The FHR pattern, the ECG complex with T/QRS analysis, and uterine contractions are recorded online on the same trace as shown in Figure 13.3.
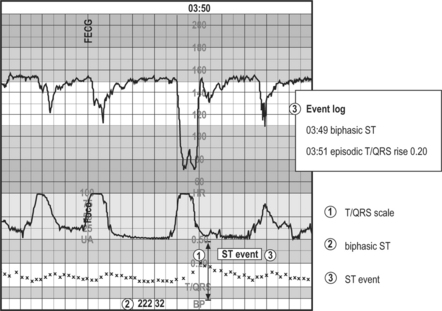
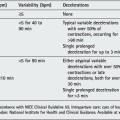
The changes in the T/QRS ratio are highlighted as STAN events on the CTG trace if they are significant, and are recorded on a log event on the screen. The early studies in the 1980s showed promising results,141, 142 but inconsistent results from other studies143 highlighted the need for computerization of ECG analysis and to take a rise in T/QRS from its own baseline levels instead of considering fixed values applicable to all fetuses. Two randomized studies, consisting of nearly 4500 subjects, based on an algorithm using the combined analysis of CTG and ECG waveform analysis (Table 13.1) have shown a reduction in the caesarean section rate and the incidence of metabolic acidosis when the ECG waveform analysis was used in conjunction with CTG, compared with CTG alone (Table 13.2).144, 145
Table 13.1 Decision-making algorithm using computerized analysis of ECG waveform with visual interpretation of the CTG
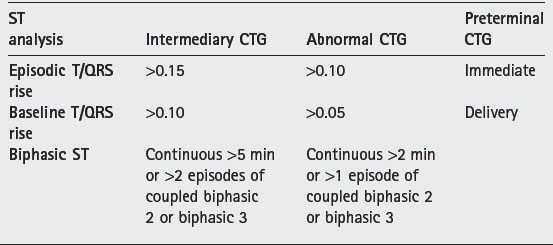
Table 13.2 The results of the Plymouth and Swedish randomized studies that show reduction in operative delivery rates for fetal distress and the incidence of metabolic acidosis at delivery144, 145
| Plymouth RCT144 | Swedish RCT145 | |
|---|---|---|
| Operative delivery for fetal distress | ||
| Control arm | 9.1% | 9.3% |
| STAN arm | 5.0% | 7.7% |
| Metabolic acidosis | ||
| Control arm | 1.40% | 1.44% |
| STAN arm | 0.55% | 0.57% |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


