Magnetic resonance (MR) imaging is the primary diagnostic imaging modality for the evaluation of patients with suspected internal derangement of the shoulder joint. Awareness and understanding of the complex anatomy of the shoulder articulation and the ability to recognize normal anatomic variants and potential imaging pitfalls are critical to accurate interpretation of conventional and arthrographic MR imaging studies. This review discusses the normal anatomy and anatomic variants of the glenoid labrum, articular cartilage, and glenohumeral ligaments. An improved understanding of normal anatomy, biomechanics, and variants will help to avoid potential pitfalls in the interpretation of noncontrast and arthrographic shoulder MR imaging examinations.
Magnetic resonance (MR) imaging is the primary diagnostic imaging modality for the evaluation of patients with suspected internal derangement of the shoulder joint. Awareness and understanding of the complex anatomy of the shoulder articulation and the ability to recognize normal anatomic variants and potential imaging pitfalls are critical to accurate interpretation of conventional and arthrographic MR imaging studies. This review discusses the normal anatomy and anatomic variants of the glenoid labrum, articular cartilage, and glenohumeral ligaments (GHLs). An improved understanding of normal anatomy, biomechanics, and variants helps to avoid potential pitfalls in the interpretation of noncontrast and arthrographic shoulder MR examinations.
Labrum
Function/Biomechanics
The glenoid labrum acts as a passive stabilizer to the glenohumeral articulation by adding depth to the shallow glenoid fossa. It also serves as a primary attachment site for the GHLs, joint capsule, and long head of the biceps tendon. The labrum demonstrates considerable anatomic variability in its appearance, which may pose a diagnostic challenge to image interpretation.
The labral outline is ovoid in configuration, conforming to the underlying glenoid rim, and is most firmly attached to the glenoid posteriorly and inferiorly. Previous reports have shown the labrum to be predominantly composed of fibrous tissue with some fibrocartilaginous components at the chondrolabral junction. At the central interface of the glenoid labrum and the glenoid cartilage, 2 specific types of chondrolabral junctions have been described. There may be an abrupt transition with the labrum demonstrating a free edge margin (type A) or there may be a transition zone where the fibrous labrum blends with the glenoid hyaline cartilage (type B attachment) ( Fig. 1 ). Initially the labrum was considered to normally be of low signal intensity on all MR pulse sequences; however, more recent studies have identified areas of increased linear or globular signal intensity in nearly a third of arthroscopically normal labral tissue. In type B attachments, intermediate signal intensity may be noted at the chondrolabral junction corresponding to the transitional zone of fibrocartilage, which should not be misinterpreted as a labral tear.

Typically considered to be triangular or rounded in cross section, a range of glenoid labral morphologies has been described. Park and colleagues evaluated labral shape on 108 arthrograms of asymptomatic volunteers and found a triangular shape to be most common (anterior, 64%; posterior, 47%) followed by rounded (17%, 33%). Flat, cleaved, notched, or absent labrum was also seen. The labrum typically measures approximately 4 mm in width and 3 mm in thickness; however, broad variation in labral size from 2 to 14 mm between normal individuals exist, thus rendering size criteria of little diagnostic utility.
Superior Labrum
The labrum demonstrates its greatest variation in morphology and attachment above the equator. At the superior labrum, fibers from the proximal origin of the long head of the biceps tendon blend with the labrum forming the biceps labral complex (BLC). Three distinct types of complexes have been described ( Fig. 2 ). In a type I BLC, the labrum is firmly attached to the glenoid rim, with no intervening cartilage or central free edge. In a type II BLC, the attachment of the glenoid labrum and biceps tendon to the glenoid occurs more medially and there is continuation of the hyaline cartilage under the labrum accompanied by a small synovial-lined sulcus between the labral free edge and cartilage. In a type III BLC, a prominent triangular meniscoid labrum projects into the joint space and results in a deep recess that may be continuous with a sublabral foramen ( Fig. 3 ).


The sublabral sulcus or recess present in type II and III BLCs represents the most frequent normal anatomic variant of the superior labrum. A cadaveric study by Smith and colleagues demonstrated a recess deeper than 2 mm to be present in 39% of specimens. The recess can be identified on routine MR imaging and is enhanced by the presence of a joint effusion or an intra-articular contrast solution. Mischaracterization of this finding as a superior labral anterior-posterior (SLAP) II tear is a potential diagnostic pitfall. Tuite and Orwin described 3 key features of the superior recess to help differentiate it from an SLAP tear: (1) location: a sulcus typically extends only to the most posterior insertion point of the biceps tendon attachment to the labrum and glenoid ; (2) contour: a sulcus should demonstrate smooth margins, any irregularity in the contour should be considered suspicious for SLAP tear; and (3) orientation: the direction of increased signal intensity/fluid should extend medially, paralleling the underlying glenoid cartilage; any extension laterally into the substance of the labrum should be considered pathologic. A shallow contrast-filled cleft can sometimes be depicted between the labrum and the biceps, the so-called bicipital labral sulcus ( Fig. 4 ).

A second normal anatomic variant of the superior labrum is the sublabral foramen that may be seen in association with a sublabral sulcus or in isolation. Present in 11% of normal patients, the foramen represents a focal developmental detachment of the anterosuperior labrum, which may be confused with an anterior labral tear if care is not taken to note features of this anatomic variant ( Fig. 5 ). Again, location is a key factor because the normal foramen is identified along the anterosuperior quadrant between the 1-o’clock to 3-o’clock position. The sublabral foramen can vary in extent from a focal detachment to involvement of the entire anterosuperior quadrant. Initial descriptions of the location of the foramen stated that it should not extend below the level of the midglenoid notch that is present at the physeal line or junction of the superior and middle thirds of the glenoid; however, Tuite and colleagues noted that in some patients a sublabral foramen may extend below the midglenoid notch. Smooth margins of the foramen, no significant displacement (<1–2 mm) of the detached labrum, and lack of associated traumatic injuries in the adjacent capsuloligamentous structures are additional helpful parameters to distinguish this variant from a labral tear. The sublabral foramen provides a communicating pathway between the glenohumeral joint and the subscapularis recess ( Fig. 6 ). Loose bodies may extrude through a sublabral foramen and collect in the subscapularis recess. Constricted joint fluid access to the subscapularis recess through the sublabral foramen should not be misconstrued as a type II SLAP tear with associated paralabral cyst. High origin of the middle and inferior GHLs (MGHL and IGHL) with narrowing of Weitbrecht foramen may promote extension of fluid and/or debris through the sublabral foramen as an alternative path to the subscapularis recess. The presence of high origin of the anterior band of the IGHL was recently reported as a potential imitator of sublabral foramen.


The anterosuperior labrum may also be diminutive or absent. The combination of an absent anterosuperior labrum and a thickened cordlike MGHL is termed the Buford complex; this is a relatively uncommon normal variant, occurring in approximately 1.5% of patients ( Fig. 7 ). This variant is important to recognize because it may also be misinterpreted as a labral tear or a displaced long head of the biceps tendon. Care should be taken to follow the cordlike structure on consecutive axial images cross-referencing them in the sagittal plane.

MR Imaging Technique
The labrum is routinely evaluated in all 3 planes on MR imaging, with the axial plane providing the most diagnostic information and the coronal plane serving an adjunctive role for evaluation of the superior labrum and inferior glenohumeral capsulolabral complex. Several reports have detailed the importance of proper shoulder positioning to optimize evaluation of its complex anatomy and specifically to aid in detection of subtle abnormalities of the glenoid labrum and GHLs. The shoulder is routinely imaged in neutral or slight external rotation. The degree of rotation can be assessed by noting the position of the bicipital grove on axial images. Significant internal rotation should be avoided for conventional MR imaging of the shoulder because it results in medial displacement of the joint capsule and contraction of the subscapularis tendon, both of which may obscure the subjacent anteroinferior labrum. MR imaging of the shoulder with the arm in alternate positions has been advocated to better assess the integrity of specific labroligamentous structures.
Abduction and External Rotation
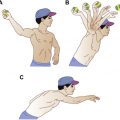
Tirman and colleagues originally described the use of abduction and external rotation (ABER) positioning for evaluation of the rotator cuff. Other investigators have since noted improved detection of anteroinferior labral pathology with the ABER technique. Imaging is performed using a flexible coil, with the arm above the head, the elbow flexed, and palm facing upward, thus placing tension on the anteroinferior capsulolabral complex and potentially revealing otherwise-occult pathology of the labrum or IGHL ( Fig. 8 ). Kwak and colleagues described the ABER position as optimal for evaluation of the IGHL and advocated it as an adjunct to routine imaging examination. In a recent publication, Schreinemachers and colleagues retrospectively compared the sensitivity and specificity of conventional arthrograms with single arthrographic series in ABER position. After reviewing 250 arthrograms with arthroscopic correlation in 92 patients, the investigators found no significant difference in detection of anteroinferior labroligamentous injury. The investigators concluded that limited study with images acquired only in the ABER position could replace the more time-consuming complete examination if there was only a clinical concern for anteroinferior labroligamentous pathology. In another recent investigation, Takubo and colleagues evaluated the nonarthrographic MR imaging technique in ABER position and found comparable sensitivity and specificity to arthroscopy for the identification of a biomechanically intact IGHL. A recognized downside to this and other adjunctive positions is prolonged examination time. In addition, some patients experience discomfort and/or a sensation of instability, particularly with the ABER position, and may not be able to tolerate this portion of the examination.

Flexion, Adduction, and Internal Rotation
Imaging of the shoulder in flexion, adduction, and internal rotation (FADIR) has been advocated to better evaluate the posterior capsulolabral complex. The FADIR position is achieved by placing the patient’s arm across the chest with the hand on the contralateral shoulder. Chiavaras and colleagues evaluated the impact of FADIR position in the detection of posterior labral tears in a recent small preliminary retrospective review and found it to be a useful adjunct to conventional imaging ( Fig. 9 ).

Adduction and Internal Rotation
Nonarthrographic MR imaging with the arm in internal rotation may cause redundancy of the anteroinferior capsular structures and obscuration of the underlying labrum, potentially leading to false-negative interpretations. With the administration of intra-articular contrast and distension of the joint, capsular apposition becomes less problematic. Song and colleagues introduced the adduction and internal rotation (ADIR) position at MR arthrography and evaluated its diagnostic performance compared with ABER and neutral position in the assessment of anterior inferior labral lesions. In their retrospective review of patients found to have anteroinferior labroligamentous injury at arthroscopy, the investigators reported that ADIR was superior to ABER and neutral position in the discrimination between subtypes of Bankart injuries.
Cartilage
Anatomy and Histology
The articular surfaces of the glenoid fossa and the humeral head are lined by hyaline cartilage. Articular congruity of the glenohumeral joint is improved by normal alterations in the cartilage thickness. There is relative thinning of the articular cartilage of the glenoid centrally and thickening along the periphery. In contradistinction, the articular cartilage of the humeral head is thicker centrally and thinner near its margins.
A focal well-demarcated articular cartilage defect at the central aspect of the glenoid termed the bare spot has been reported in the surgical and radiologic literature ( Fig. 10 ). Burkhart and colleagues reported its consistent location at the central aspect of the inferior glenoid and noted that it provided a useful landmark at arthroscopy to quantify the degree of glenoid bone loss. However, in a subsequent study by Kralinger and colleagues in which 3-dimensional computed tomography of cadaveric specimens was performed, the investigators discovered variation in the location of the bare spot. Evaluation in the pediatric population using MR imaging has also shown some slight but significant variability in the location of the bare spot. Kim and colleagues also noted a considerable lower incidence in the pediatric population supporting the hypothesis that this may be an acquired finding.
Focal thickening of the subchondral bone along the central aspect of the glenoid fossa is an additional normal variant termed the Ossaki tubercle. This is typically accompanied by thinning of the overlying cartilage. These variants should not be mischaracterized as osteochondral injuries. The absence of subchondral bone marrow signal abnormality and lack of intra-articular loose bodies are pertinent negative findings.
A bare area of the humeral head devoid of articular cartilage or sulcus has also been described. Located posteriorly between the posterior insertion of the joint capsule and synovial membrane and the adjacent articular cartilage, this bare area may be confused with a Hill-Sachs impaction injury ( Fig. 11 ). An additional bare area has been described between the supraspinatus insertion on the greater tuberosity and the adjacent articular cartilage. This bare area is used by surgeons to quantify partial-thickness articular surface tears. Failure to recognize and account for the bare area at imaging may lead to erroneous diagnosis or overestimation of partial thickness supraspinatus tendon tears. In contradistinction, widening of the bare area may be due to loss of the articular cartilage and/or undersurface supraspinatus tear.
Related posts:
 Magnetic Resonance Imaging of Rotator Cuff Disease and External Impingement
Magnetic Resonance Imaging of Rotator Cuff Disease and External Impingement
 Internal Impingement Syndromes
Internal Impingement Syndromes
 The Throwing Shoulder: the Orthopedist Perspective
Postoperative Shoulder Magnetic Resonance Imaging
Magnetic Resonance Imaging of the Pediatric Shoulder
The Throwing Shoulder: the Orthopedist Perspective
Postoperative Shoulder Magnetic Resonance Imaging
Magnetic Resonance Imaging of the Pediatric Shoulder
 Entrapment Neuropathies of the Shoulder
Entrapment Neuropathies of the Shoulder
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


