Internal causes of impingement are secondary to rotator cuff and capsular dysfunction and are categorized by the location of the impingement and the underlying pathophysiological or mechanical cause of the impingement. These include posterosuperior impingement, anterosuperior impingement, anterior impingement, and entrapment of the long head of the biceps tendon. The objective of this article is to review magnetic resonance imaging findings of each of the 4 types of internal impingement syndromes and discuss the pathophysiology behind the impingement.
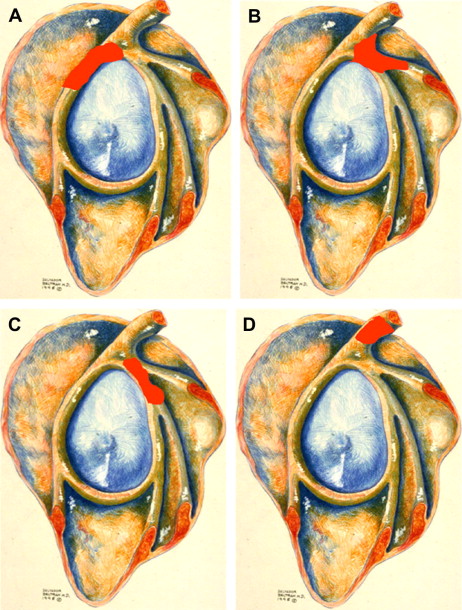
Impingement syndromes of the shoulder can be caused by external or internal causes. External causes are due to primary abnormalities in the coracoacromial arch causing extrinsic compression of the subacromial bursa and the rotator cuff, leading to rotator cuff tear and retraction, as first described by Neer in 1972, and including subacromial and subcoracoid impingement. It occurs most commonly in middle-aged nonathletic individuals. Internal causes of impingement are secondary to rotator cuff and capsular dysfunction and are categorized by the location of the impingement and the underlying pathophysiological or mechanical cause of the impingement. These include posterosuperior impingement, anterosuperior impingement, anterior impingement, and entrapment of the long head of the biceps tendon (LHBT) ( Fig. 1 ). Although the diagnosis of internal impingement is primarily clinical, magnetic resonance imaging (MRI) can play an important role in confirming clinical suspicion or suggesting the diagnosis. In this article, the authors discuss the MRI evaluation and pathophysiological mechanisms of internal impingement syndromes of the shoulder.
Posterosuperior impingement
Posterosuperior impingement, which was first described by Walch and colleagues, refers to contact of the undersurface of the posterosuperior rotator cuff with the posterosuperior labrum when the arm is abducted and externally rotated (ABER), where the cuff can become pinched between the labrum and the greater tuberosity. It occurs most frequently in professional throwing athletes and is attributed to repetitive overhead motion, most commonly in baseball pitchers, tennis players, javelin throwers, and swimmers. Typical symptoms include posterior superior shoulder pain that commences during the late cocking phase of overhead movement and intensifies during the early acceleration phase.
Jobe presented an expanded spectrum of injury occurring in overhead throwing athletes in the setting of posterosuperior impingement, which includes injuries to the superior labrum, the rotator cuff tendon, the greater tuberosity, the inferior glenohumeral ligament, and the superior glenoid bone. He also suggested that internal impingement in throwing athletes may progressively worsen because of gradual stretching of the anterior capsuloligamentous structures, leading to anterior displacement of the humeral head and impingement of the rotator cuff and the posterosuperior labrum between the greater tuberosity of the humerus and the glenoid margin. This theory led to the initial treatment approach for anterior glenohumeral instability using anterior capsulolabral reconstruction; however, results of this treatment were unpredictable. Halbrecht and colleagues disagreed with Jobe’s premise of anterior instability worsening internal impingement and showed that glenohumeral instability, where the humeral head is subluxed anteriorly, resulting in decreased contact with the posterosuperior glenoid compared with the reduced position. Therefore, they proposed that anterior instability does not worsen internal impingement but rather lessens it. The role of anterior capsular laxity as a causative factor in posterosuperior impingement is still controversial.
Burkhart and colleagues proposed that posterosuperior impingement is a normal phenomenon in all shoulders and is not usually pathologic in the disabled throwing shoulder. Rather they proposed that scarring of the posterior joint capsule leads to loss of internal rotation of the humeral head in the throwing athlete, starting a pathologic cascade that results in posterosuperior shift of the glenohumeral rotation point during abduction and external rotation that is maximal in the late cocking phase of throwing. The posterosuperior displacement of the rotation point may be also caused by the thickened posterior capsule moving inferior to the humeral head on abduction and external rotation, according to Burkhart and colleagues. At this point the shift results in maximal shear stress on the posterosuperior labrum and the biceps anchor, resulting in a peel back mechanism that produces a posterior type IIB superior labrum anterior and posterior (SLAP) lesion with posterior extension. This is also referred to as glenohumeral internal rotation deficit (GIRD), because it is believed that the primary initiating event of this cascade of events is scarring of the posterior joint capsule leading to restriction of internal rotation or excessive external rotation. Throwing athletes with GIRD require an increase of the external rotation during the late cocking phase to achieve sufficient throwing power ( Fig. 2 ).
Related posts:
 Magnetic Resonance Imaging of Rotator Cuff Disease and External Impingement
Magnetic Resonance Imaging of Rotator Cuff Disease and External Impingement
 The Throwing Shoulder: the Orthopedist Perspective
The Throwing Shoulder: the Orthopedist Perspective
 The Rotator Cable: Magnetic Resonance Evaluation and Clinical Correlation
Magnetic Resonance Imaging of the Pediatric Shoulder
The Rotator Cable: Magnetic Resonance Evaluation and Clinical Correlation
Magnetic Resonance Imaging of the Pediatric Shoulder
 Entrapment Neuropathies of the Shoulder
Entrapment Neuropathies of the Shoulder
 Anatomic Variants and Pitfalls of the Labrum, Glenoid Cartilage, and Glenohumeral Ligaments
Anatomic Variants and Pitfalls of the Labrum, Glenoid Cartilage, and Glenohumeral Ligaments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


