22
Anatomy of the Kidneys and Genitourinary Tract
The urinary system comprises the upper urinary tracts (kidneys and ureters), the urinary bladder, and the urethra. The genital system consists of the testes, epididymides, deferent ducts, seminal vesicles, ejaculatory ducts, the prostate, and the penis in males; and the ovaries, uterine tubes, uterus, and vagina in females. A complete review of the embryology and anatomy is beyond the scope of this book; instead, an overview is given from the perspective of the vascular and interventional radiologist (VIR). The emphasis, therefore, is on the urinary system and the uterine tubes, which provide a fertile ground for interventional procedures. Anatomy of the penis is more appropriately discussed in Chapter 2. Embryology is presented for a better understanding of the anatomy and of the more frequently encountered variants and anomalies.
 Embryology
Embryology
The urinary tract develops in three overlapping stages: the pronephros, the mesonephros, and the metanephros (Fig. 22-1).1 Development progresses from the cranial aspect toward the cloaca. As the more caudal segments develop, the earlier, cranial ones involute. The pronephros does not have an excretory function in the human and involutes completely. The mesonephros is constituted by a pair of medially located mesonephric ducts (wolffian ducts) and laterally located nephrogenic cords. The nephrogenic cords form a collection of glomeruli and primitive tubules connected to the mesonephric ducts. The mesonephric duct eventually extends caudally and establishes a communication with the cloaca, allowing excretion of urine. Unlike the pronephros, some of the mesonephric remnants participate in the formation of the adult male genital tract (efferent ductules, epididymis, paradidymis, vas deferent, seminal vesicles, and ejaculatory ducts). The metanephros develops from two separate components: the metanephric duct (ureteral bud) and the metanephric blastema. The ureteral bud is a small outpouching that arises from the caudal aspect of the mesonephric (wolffian) duct in approximately the 5-week-old embryo. This bud grows ventrally and superiorly, forming a long tube with a dilated cranial blind end, called the ampulla. Surrounding the ampulla of the metanephric duct on each side is a cellular mass called the metanephric blastema. As the metanephric ducts elongate, they also divide and penetrate the blastema, inducing differentiation.
As the ureteral bud lengthens, the lumbosacral region of the embryo undergoes accelerated growth. The combination of these processes results in an apparent ascension of the kidneys from the initial caudal origin toward their final position in the midabdomen. Concomitant with this apparent cranial migration, the kidneys also rotate medially, which results in the final position at birth, with the excretory portion of the kidney being lateral and the renal pelvis located medially. Failure of these processes results in a variety of abnormalities of size, shape, position, and number of the kidneys. Frequently, these anomalies coexist. For example, in the horseshoe kidney (the most frequent fusion anomaly, where the lower poles of the kidneys are fused across the midline), the renal pelves are ventral because of the absence of normal rotation, the kidney is lower than normal (ectopic), and the arterial supply is commonly aberrant (multiple renal arteries originating from the distal aorta and the iliac arteries). During ascension, the kidneys are supplied with blood by paired mesonephric branches of the aorta. As kidneys ascend, branches arising at lower levels involute and more cranial branches substitute for them. Failure of this involution results in accessory or aberrant renal arteries (25% of normal); these arteries are usually lower and of smaller caliber than the main renal arteries and supply the polar regions.
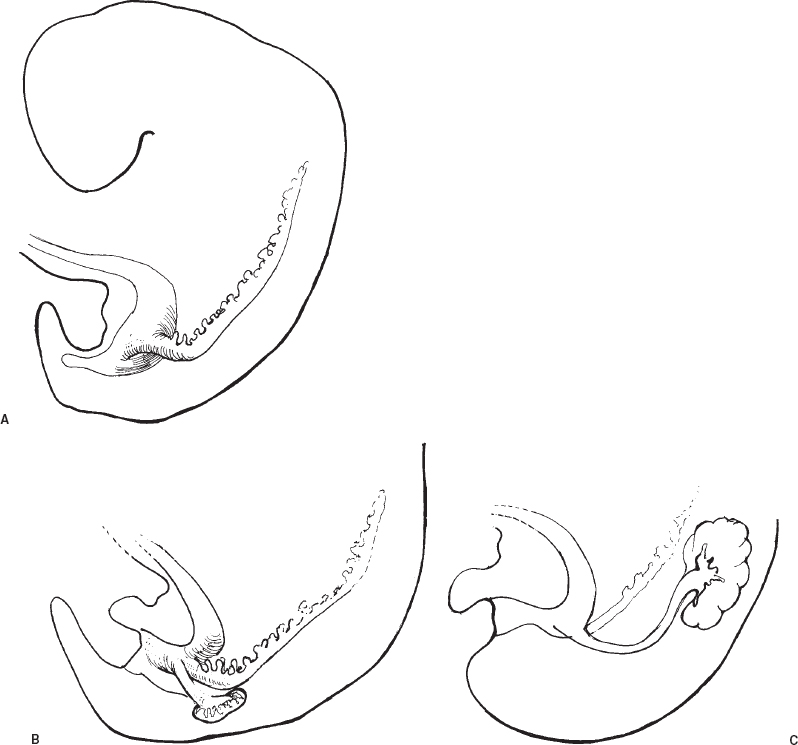
FIGURE 22-1. A: Pronephros (2nd through 6th somites) and early mesonephros; approximately 3 weeks. B: Mesonephros (9th through 16th somites) and early metanephros; 3+ weeks. C: Metanephros and apparent renal migration; 5 weeks to term. Note the complete degeneration of the pronephros and partial degeneration of the mesonephros.
Renal ontogenesis concludes with the process of maturation, which entails the overall growth of the organ and variable degree of fusion of the approximately 14 initiallobes (seven ventral, seven dorsal)(Fig. 22-2A).2 A result of this lobar fusion is the smoothing of the renal surface with effacement of interlobar septations (Fig. 22-2B). This process is more pronounced at the poles than at the interpolar region (Fig. 22-3). Another consequence of the lobar fusion is the formation of compound calyces. This process is also more pronounced in the polar regions; therefore, the upper and lower pole calyces tend to be compound, whereas the interpolar calyces usually maintain their original ventral and dorsal distribution. The implications of lobar fusion for the VIR will be further discussed in the subsection on renal anatomy.
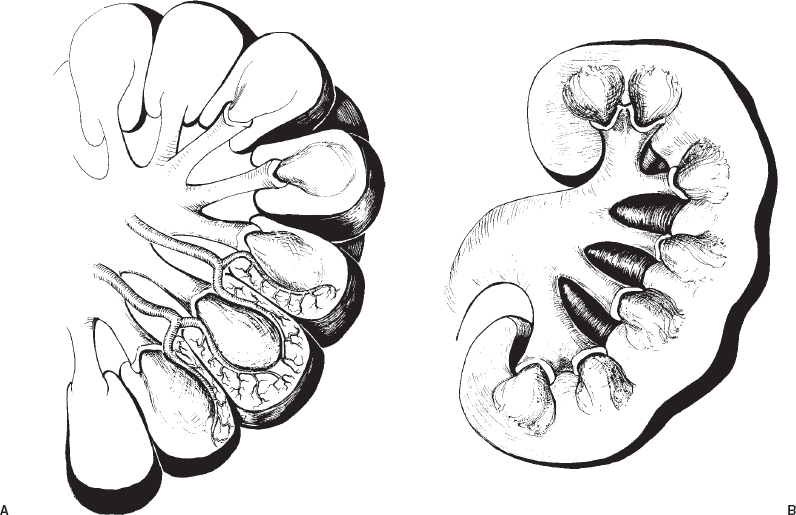
FIGURE 22-2. A: Diagram of the fetal kidney at approximately 28 weeks (coronal section). On average, there are 14 lobes (7 ventral and 7 dorsal), each irrigated by at least two interlobar arteries. The lobes are separated by connective tissue planes and demarcated by deep grooves on the surface of the kidney. B: Fetal kidney at term (coronal section).Variable degree of lobar fusion results in compound calices and effacement of the surface grooves.

FIGURE 22-3. Marked bilateral fetal lobulation of the kidneys (left greater than right); abdominal aortogram, late venous phase. Note the predominance in the interpolar area (right).
 Anatomy
Anatomy
Kidneys
Good knowledge of renal anatomy is a prerequisite for percutaneous access to the renal collecting system, a well-established procedure performed for relief of obstruction or as a preamble for other diagnostic or therapeutic procedures (biopsy, diversion of the urinary stream, stricture treatment, ureteral occlusion, or percutaneous stone extraction).
The mature kidneys are paired organs. The left is usually slightly larger than the right, and there is significant individual variation in size; however, as an overall rule, kidney size is relatively symmetric (Fig. 22-4). The kidneys are bean shaped with a medial indentation called hilum. The contours are variably smooth, depending on the degree of lobar fusion. Contours can be deformed by indentation by adjacent organs, most frequently in the left kidney, secondary to splenic impression (Fig. 22-5). Normally, the kidneys are located at the level of the twelfth thoracic to the third lumbar vertebrae. The left kidney is usually slightly higher than the right. Both kidneys are mobile and can change position significantly, both with the phase of respiration and with change in position of the patient.3 This mobility can be used to the advantage of the VIR because a needle inserted percutaneously into the kidney will swing characteristically with respiratory motion, whereas an extrarenal needle will not change position appreciably with respiratory motion.

FIGURE 22-4. Normal urogram. Note the symmetry of the shape and size of the kidneys, the higher position of the left kidney, and the compound calices in the polar areas. Some asymmetry can be seen in the morphology of the pelves.
Both kidneys are retroperitoneal organs. The retroperitoneal space is delineated anteriorly by the parietal peritoneum, posteriorly by the fascia transversalis, superiorly by the diaphragm, and inferiorly by the pelvic brim. The retroperitoneal space is subdivided in three important compartments (Fig. 22-6).4 The anterior pararenal space is delineated by the parietal peritoneum and posteriorly by the anterior renal fascia (Gerota’s fascia). This space contains the ascending and descending colon, the pancreas, duodenum, and a small amount of retroperitoneal fat. The two sides of the anterior pararenal space are continuous across the midline, and there is potential communication with the posterior pararenal space inferiorly.

FIGURE 22-5. Splenic impression on the left kidney (arrow) ; abdominal aortogram, late venous phase.
The perirenal space is delineated anteriorly by the anterior renal fascia and posteriorly by the posterior renal fascia (fascia of Zuckerkandl). It contains the kidneys, adrenal glands, ureters, abundant perirenal fat, and the great vessels (aorta and the inferior vena cava). The peri-renal fat is continuous with the renal sinuses. The perirenal space does not communicate across the midline and therefore has two separate compartments (right and left). A strong, fibrous, nonadherent capsule envelopes each kidney, separating it from the perirenal fat. This capsule and the thoracolumbar fascia (aponeurosis of transverse abdominal muscle) are the points where a needle meets resistance during percutaneous puncture of the renal collecting system.2
The posterior pararenal space is bordered anteriorly by the posterior renal fascia and posteriorly by the fascia transversalis. This space contains only fat. It communicates potentially with the anterior pararenal space at the pelvic rim and with the mediastinum superiorly through the paravertebral space. The importance of the retroperitoneal space divisions lies in the characteristic radiological findings of fluid or gas collections within each of these compartments.
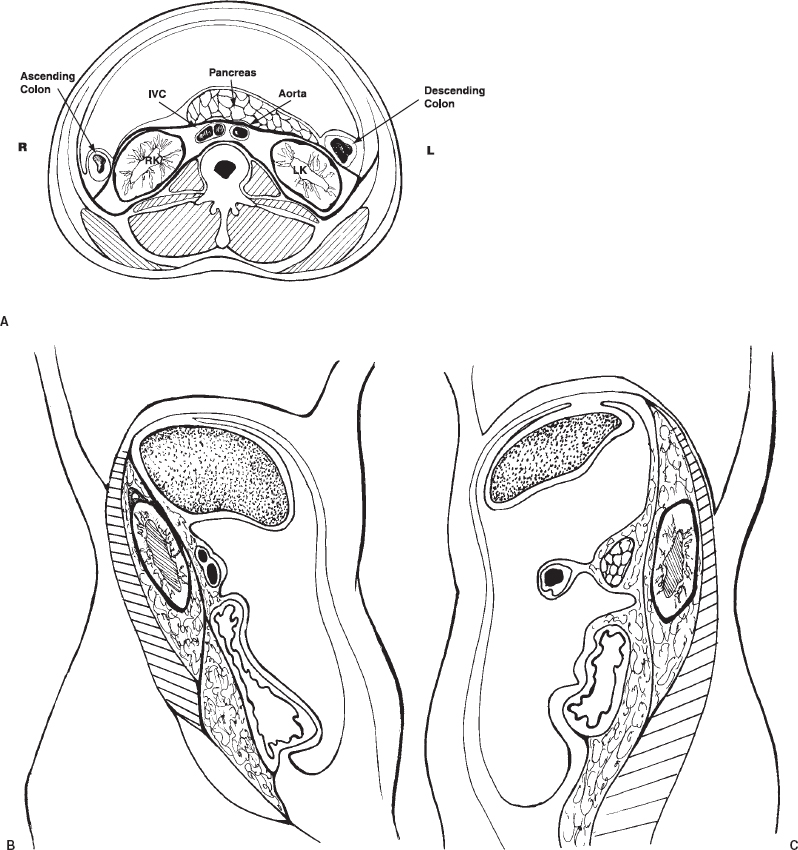
FIGURE 22-6. Axial (A) and right (B) and left (C) parasagittal diagramatic sections through the abdomen, illustrating the retroperitoneal compartments. The anterior pararenal space contains the pancreas, ascending and descending colon and the duodenum. The perirenal space contains the kidneys, ureters and adrenal glands. The posterior pararenal space contains fat. Note rotation of the kidneys about the longitudinal and transverse axes. From Castaneda-Zuniga, WR, Tadavarty SM, eds. Interventional radiology, 2nd ed. Baltimore: William & Wilkins, 1992.
Posterior relationships of the kidneys within the renal fossa are important for the understanding and planning of percutaneous procedures.5 Superficially, a muscle layer formed by the quadratus lumborum muscle laterally and the psoas muscle medially extends from the costal margin to the iliac crest. Superiorly, the posterior aspect of the diaphragm comes in relationship with the upper poles of the kidneys. The aponeurosis of the transverse abdominal muscle completes the posterior wall of the abdomen. Because of the slightly higher position of the left kidney, it is crossed posteriorly by the eleventh and the twelfth ribs, whereas usually the right kidney comes in posterior contract with only the twelfth rib. As mentioned, the position of the kidneys and their mobility with respiratory motion will vary significantly. As a result, the posterior pleural space may be traversed during an attempted upper pole (intercostal) percutaneous puncture. Because such punctures sometimes are required by the clinical situation, care must be taken to ensure an extrapleural tract by careful fluoroscopic examination with steep oblique or lateral projections or by cross-sectional studies [computed tomography (CT) scan].2 Transpleural punctures can result in significant complications such as pneumothorax, hydrothorax, or hemothorax. Also noteworthy is the need to avoid the intercostal vessels, which course along the inferior groove of the ribs. Therefore, intercostal punctures should be performed with the needle hugging the superior aspect of the rib.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


