The lower limb is encased in a dense layer of connective tissue—the deep fascia—that acts to contain the leg muscles and improve venous flow as the muscles contract. In the lateral aspect of the thigh, the fascia is thickened and forms the iliotibial tract. This tract is a conjoint aponeurosis of the gluteus maximus and tensor fasciae latae. The distal portion of the iliotibial tract is attached to the lateral condyle of the tibia.
Septae from the deep fascia separate the thigh muscles into three compartments. The lateral intermuscular septum between the anterior and posterior groups is thicker and stronger than the other two septa. At the knee, the subcutaneous fascia and deep fascia merge, but in the thigh and calf there is fatty connective tissue between the superficial and deep fascia. The superficial veins, cutaneous nerves, and lymphatics lie in this subcutaneous tissue.
In the calf, the fascia is called the crural fascia, and it also separates the deep and superficial posterior muscles. The interosseous membrane and the crural intermuscular septa separate the anterior, extensor, and posterior muscle groups. In the lower portion of the calf, the crural fascia forms the extensor retinaculum. Accumulation of excess fluid in a compartment may compromise both nerve and vascular supply to muscles within the compartment.
The saphenous opening is a deficiency in the fascia lata inferior to the medial part of the inguinal ligament over the upper portion of the femoral triangle. The opening has a well-defined crescentic margin, except on its medial aspect. A thin connective tissue—the cribriform fascia—covers the opening. The long saphenous vein and lymphatics pass through the fascia and enter the femoral triangle.
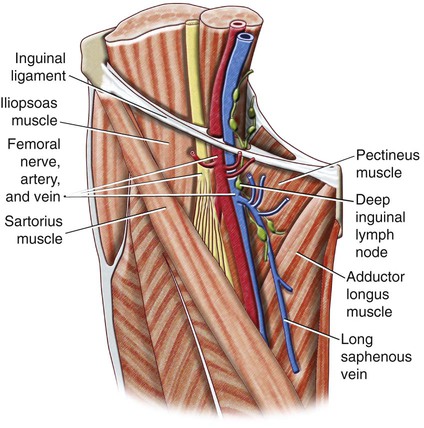
The femoral triangle is a space in the upper part of the thigh that is bounded above by the inguinal ligament, medially by the adductor longus, and laterally by the sartorius muscles (Fig. 31-1). The floor of the triangle is formed by the iliopsoas laterally and the pectineus medially. The roof of the triangle is composed of the cribriform fascia and fascia lata, subcutaneous tissue, and skin. The contents of the triangle are, from lateral to medial, the femoral nerve and its branches, the femoral artery and its branches, the femoral vein and its proximal tributaries, including the long saphenous vein and the deep inguinal lymph node, and associated lymphatics.
The femoral vein and artery and the lymphatics, but not the femoral nerve, are enclosed in the femoral sheath, which is an extension of the extraperitoneal fascia overlying the iliopsoas and transversalis abdominis. The femoral sheath is further divided into compartments for the femoral artery, femoral vein, and lymphatics. At the inferior extent of the femoral triangle the sheath becomes continuous with the adventitia of the vessels. The medial compartment is called the femoral canal, and its proximal extent under the inguinal ligament is termed the femoral ring. This opening is usually closed by fibrofatty tissue and is the site of a femoral hernia should one develop (Fig. 31-2).
The femoral nerve is the largest branch of the lumbar plexus and is composed of sensory and motor fibers from L2 to L4. It is formed within the psoas and enters the femoral triangle at about the midpoint of the inguinal ligament. Within the triangle, the femoral nerve divides into multiple branches to the quadriceps, sartorius, and the hip and knee joints. Its cutaneous branches supply the skin on the anterior and medial aspect of the thigh. Its largest cutaneous branch—the saphenous nerve—runs obliquely downward in the femoral triangle to lie adjacent to the femoral artery and vein. The saphenous nerve then passes into the adductor canal and exits proximal to the adductor hiatus by passing superficially between the gracilis and sartorius. The saphenous nerve passes along the anteromedial aspect of the calf close to the long saphenous nerve to supply skin on the anteromedial aspect of the calf and foot. At the medial malleolus, it may be damaged by a cutdown for access to the long saphenous vein.
The femoral artery arises as a continuation of the external iliac artery beneath the inguinal ligament. In the femoral triangle, it lies centrally between the femoral nerve and vein. It enters the adductor canal and continues as the popliteal artery once it passes through the adductor hiatus to the popliteal fossa. The femoral artery gives off the superficial epigastric artery, superficial circumflex iliac artery, and superficial and deep external pudendal arteries in the upper portion of the triangle before it gives off the deep artery of the thigh (profunda femoris) and continues as the (superficial) femoral artery in the adductor canal (Fig. 31-3). Within the canal, the femoral artery gives off several muscular branches and the descending genicular artery. The proximal superficial branches of the femoral artery are important collateral pathways in the event of arterial occlusion.
Branching variations at the origin of the deep artery of the thigh are common, and the length of the (common) femoral artery before the origin of the deep artery of the thigh is variable. Occasionally, the deep artery of the thigh is absent and replaced by direct branches from the femoral artery. Rarely, the anterior division of the internal iliac artery may continue from the pelvis as the sciatic artery, which terminates as the popliteal artery. In such cases, the femoral artery is small and supplies only the upper part of the thigh.
The deep artery of the thigh lies posterior to the femoral artery and passes deeply between the pectineus and adductor longus. Proximally, the deep artery of the thigh gives off medial and lateral circumflex femoral branches that form the cruciate anastomosis with obturator branches of the inferior gluteal and superficial circumflex femoral arteries. The cruciate anastomosis often supplies a branch to the sciatic nerve. Sometimes the obturator artery or an accessory obturator artery arises as a branch of the inferior epigastric artery. In this case, the artery lies on the femoral ring and may become incorporated in a femoral hernia.
The muscular branches of the deep artery of the thigh provide large collateral opportunities when there is occlusion of the femoral artery in the adductor canal. The medial circumflex femoral artery is the major supply to the head of the femur.
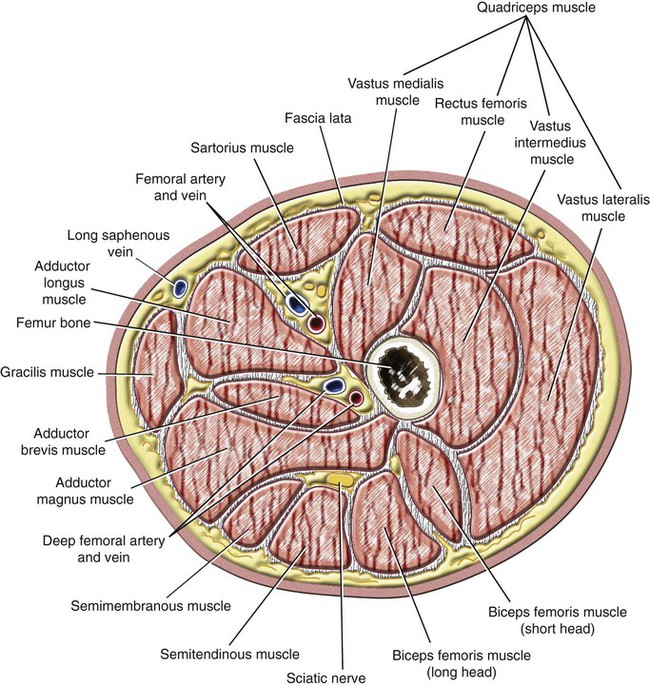
The adductor canal is a narrow space deep to the sartorius and bounded anteriorly and laterally by the posterior aspect of the vastus medialis and posteriorly by the adductor longus and adductor magnus. It contains the saphenous nerve, the (superficial) femoral artery, and the femoral vein. The adductor hiatus is an opening between the distal attachments of the adductor magnus immediately above the adductor tubercle of the femur.
The femoral vein
Only gold members can continue reading.
Log In or
Register to continue

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree