CORRECTED TRANSPOSITION
OF THE GREAT ARTERIES
 COMPLETE TRANSPOSITION OF THE GREAT ARTERIES
COMPLETE TRANSPOSITION OF THE GREAT ARTERIES
Definition, Spectrum of Disease, and Incidence
Complete transposition of the great arteries (TGA) is a common cardiac malformation, with atrioventricular concordance and ventriculoarterial discordance. This implies a normal connection between the atria and ventricles; the right atrium is connected to the right ventricle through the tricuspid valve and the left atrium is connected to the left ventricle through the mitral valve, but there is a switched connection of the great vessels, the pulmonary artery arising from the left ventricle and the aorta arising from the right ventricle. Both great arteries display a parallel course, with the aorta anterior and to the right of the pulmonary artery (Fig. 20-1), hence the term D-TGA (D = “dexter”). D-TGA is a relatively frequent cardiac anomaly occurring in 5% to 7% of all congenital cardiac malformations, with an incidence of 0.315 cases per 1000 live births and a 2:1 male preponderance (1,2). D-TGA can be an isolated cardiac malformation, termed simple D-TGA, or complex, when associated with other cardiac anomalies. Ventricular septal defects and pulmonary stenosis (left ventricular tract outflow obstruction) are common associations with D-TGA and may be present either alone or in combination in up to 30% to 40% of cases (3,4). Associated extracardiac malformations are rare.
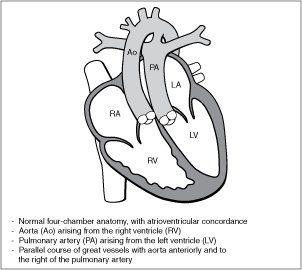
Figure 20-1. Complete transposition of the great arteries (D-TGA). RA, right atrium; LA, left atrium.
Prenatal diagnosis of D-TGA is still a challenge. Prenatal screening policy for congenital heart disease, which primarily focuses on the four-chamber view alone, will undoubtedly fail in detecting TGA. Prenatal screening for congenital heart disease at a population level reports detection rates of 3% to 17% for simple TGA (5–7). The detection rate of TGA increased from 12.5% to 72.5% during a period of rapid progress and increased access to prenatal diagnosis in a population-based study (8). Given an associated decrease in neonatal morbidity and mortality in prenatally detected TGA, assessment of the great vessels as part of the extended basic cardiac examination of the fetus should be performed when feasibly achievable (8–10). Figure 20-2 shows an anatomic fetal specimen of a heart with TGA.
Ultrasound Findings
Gray Scale
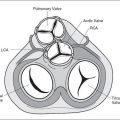
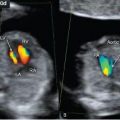
The four-chamber view is typically normal in fetuses with D-TGA (Fig. 20-3A), except for an associated ventricular septal defect. Visualization of the five-chamber view will show the pulmonary artery arising from the left ventricle and bifurcating, shortly after its origin, into two branches: right and left pulmonary arteries (Fig. 20-3B). The aorta is noted to arise from the right ventricle in an anterior and parallel course to the pulmonary artery. This parallel orientation of the great arteries in D-TGA is best obtained in an oblique plane of the heart, spatially oriented from the right shoulder to the left hip of the fetus (Fig. 20-4A,B). A transverse view in the upper thorax will show, instead of the three-vessel-trachea view in most cases, a single large vessel (the transverse aortic arch) with a superior vena cava to its right (Fig. 20-5A,B). The large vessel noted in the three-vessel-trachea view is the aorta, which is positioned anteriorly and superiorly to the pulmonary artery. The short-axis view at the level of the great vessels shows both the aorta and pulmonary artery as circular structures adjacent to each other (Fig. 20-6B) instead of their normal orientation (longitudinal pulmonary artery wrapping around a circular aorta) (Fig. 20-6A). On longitudinal views, the aortic arch is seen arising from the anterior right ventricle, giving rise to head and neck vessels and assuming a
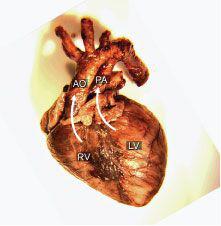
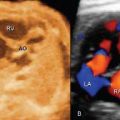
Figure 20-2. Anatomic specimen of a fetal heart with D-transposition of the great arteries. Note the aorta (AO) arising from the right ventricle (RV), anterior and parallel to the pulmonary artery (PA), which arises from the left ventricle (LV). Compare with an anatomic specimen of a normal heart in Figure 4-4.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


