Ankle Ultrasound

Clinical photograph shows the patient position for scanning the anterior ankle. The patient lies on the examination couch with the knee flexed and the sole of the foot resting on the couch.

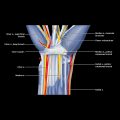
Longitudinal US of the midline anterior aspect of the ankle joint  shows the distal tibia
shows the distal tibia  , anterior capsule
, anterior capsule  , intraarticular extra synovial fat pad
, intraarticular extra synovial fat pad  , and articular cartilage covering the talar dome
, and articular cartilage covering the talar dome  . The anterior ankle joint should be scanned from medial to lateral.
. The anterior ankle joint should be scanned from medial to lateral.

Transverse US just proximal to ankle joint shows the tibialis anterior  and extensor hallucis longus
and extensor hallucis longus  tendons lying deep to the superior band of the extensor retinaculum
tendons lying deep to the superior band of the extensor retinaculum  .
.

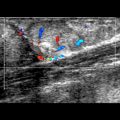
Transverse US shows the extensor digitorum longus tendon  at the level of the ankle joint just deep to the extensor retinaculum
at the level of the ankle joint just deep to the extensor retinaculum  . The tendon has just divided into its digital slips. Note the proximity of the lateral aspect of the ankle
. The tendon has just divided into its digital slips. Note the proximity of the lateral aspect of the ankle  to the skin. This makes the lateral ankle a preferred site for intraarticular injection.
to the skin. This makes the lateral ankle a preferred site for intraarticular injection.
GENERAL CONSIDERATIONS
Clinical Indications for Ankle US
TECHNIQUE: ANTERIOR ANKLE
Patient Position
Specifically Examine
 Seen on anteromedial aspect of ankle to be ~ 2x as large as other extensor tendons; ovoid-shaped as opposed to more flattened shape of other extensor tendons
Seen on anteromedial aspect of ankle to be ~ 2x as large as other extensor tendons; ovoid-shaped as opposed to more flattened shape of other extensor tendons
 Proximally, TA tendon has tenosynovium whereas distally it has paratenon
Proximally, TA tendon has tenosynovium whereas distally it has paratenon
 In 25% of patients, superior extensor retinaculum splits into 2 to form separate TA tunnel
In 25% of patients, superior extensor retinaculum splits into 2 to form separate TA tunnel
 Scan distal insertion of TA tendon in longitudinal plane with foot slightly everted
Scan distal insertion of TA tendon in longitudinal plane with foot slightly everted
TECHNIQUE: MEDIAL ANKLE
Patient Position
Specifically Examine
 Lies posterior and inferoposterior to medial malleolus bounded superficially by flexor retinaculum
Lies posterior and inferoposterior to medial malleolus bounded superficially by flexor retinaculum
 Contains “Tom (tibialis posterior), Dick [flexor digitorum (FD)], and a very nervous (artery, vein, tibial nerve) Harry [flexor hallucis longus (FHL)]”
Contains “Tom (tibialis posterior), Dick [flexor digitorum (FD)], and a very nervous (artery, vein, tibial nerve) Harry [flexor hallucis longus (FHL)]”
 Tibial nerve lies alongside posterior tibial artery and veins between FD and FHL
Tibial nerve lies alongside posterior tibial artery and veins between FD and FHL
 Compression of tibial nerve within confines of tarsal tunnel leads to tarsal tunnel syndrome
Compression of tibial nerve within confines of tarsal tunnel leads to tarsal tunnel syndrome
 Small medial calcaneal nerve arises from tibial nerve or lateral plantar nerve proximal to, within, or distal to tarsal tunnel
Small medial calcaneal nerve arises from tibial nerve or lateral plantar nerve proximal to, within, or distal to tarsal tunnel
 In 80% of patients, tibial nerve divides in tarsal tunnel into medial and lateral plantar nerves
In 80% of patients, tibial nerve divides in tarsal tunnel into medial and lateral plantar nerves
 Scan primarily in transverse plane from supramalleolar region to insertion
Scan primarily in transverse plane from supramalleolar region to insertion
 Inspect supra-, retro-, infra-, and premalleolar segments keeping transducer at right angles to tendon
Inspect supra-, retro-, infra-, and premalleolar segments keeping transducer at right angles to tendon
 TP tendon lies in shallow groove behind medial malleolus, which acts as pulley
TP tendon lies in shallow groove behind medial malleolus, which acts as pulley
 Covered by thick flexor retinaculum with hyaline cartilage more deeply (pulley enthesis)
Covered by thick flexor retinaculum with hyaline cartilage more deeply (pulley enthesis)
 Normally, TP is ~ 2x size of FD tendon
Normally, TP is ~ 2x size of FD tendon
 Small TP tendon sheath effusion is normal
Small TP tendon sheath effusion is normal
 Insertional area best seen on longitudinal scanning
Insertional area best seen on longitudinal scanning
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree