(1)
Department of Pediatric Radiology, University of Texas Medical Branch, Galveston, TX, USA
Abstract
The cervical spine, especially the upper cervical spine, is prone to numerous anomalies which can be misinterpreted for pathology. These are dealt with in detail throughout the chapter, and the focus of the chapter is on how to differentiate anomalies from pathology.
Fusion–Segmentation Anomalies
Occurring alone or as part of some syndrome, fusion–segmentation anomalies range from hemivertebra through cleft vertebrae to absence of a vertebral body. The embryology of these anomalies is presented in Chap. 1 (Figs. 1.2 and 1.3).
Midline vertebral body clefts usually are of no serious clinical consequence and are manifest primarily as butterfly or cleft vertebrae (Fig. 3.1). Most often no associated problem exists, but occasionally one can encounter such vertebrae with neurenteric or enteric duplication cysts. Sagittal hemivertebrae usually are associated with focal scoliosis (see later: Fig. 3.8). Coronal cleft and coronal hemivertebrae are less common, but the latter, especially when the anterior half of the vertebra is missing, can lead to spine instability (Fig. 3.2a, b). Finally, the entire vertebral body or bodies may be hypoplastic or absent [1], and again instability usually is present (Fig. 3.2c). Coronally cleft vertebrae are more common in the thoracolumbar spine, can be seen in syndromes such as trisomy 13–15 and rhizomelic punctate epiphyseal dysplasia and also are more common in males than in females [2]. They are, however, uncommonly encountered in the cervical spine.
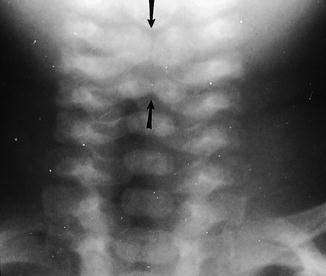

Fig. 3.1
Butterfly vertebra. Note central vertebral body narrowing (arrows), resulting in a butterfly vertebra
Fig. 3.2
Coronal segmentation anomalies and absent vertebrae. (a) Coronal hemivertebra. The anterior portion of the fourth cervical vertebra did not develop, resulting in a small vertebral body (coronal hemivertebra) and marked kyphosis at the C3–C4 level (arrow). (b) Sagittal reconstructed CT study demonstrates similar findings (arrow). (c) Absent vertebral body. In this patient the entire vertebral body of C3 is markedly underdeveloped and virtually absent (arrow). In addition, while the pedicles are developed, the posterior neural arch is not. Posterior neural arch underdevelopment also is present at the C4 and C5 levels
Fusion Anomalies of Vertebral Bodies
Fusion anomalies most commonly occur at the C2–C3 level, and such fusion frequently involves the associated apophyseal joints (Fig. 3.3). Fusion also can occur at lower levels and may be multiple (Fig. 3.4). In all these cases, the intervening disk may be completely obliterated or variably narrowed (Fig. 3.4). In addition, the involved vertebral bodies tend to taper toward the rudimentary disk (Fig. 3.4); interestingly, the disks above and below the level of fusion often are enlarged or hypertrophied. This is important to appreciate, for unless cord compression is seen these hypertrophied disks should not be interpreted as representing pathologic degeneration and herniation. This manifestation of vertebral fusion is best demonstrated with MRI (Fig. 3.5).

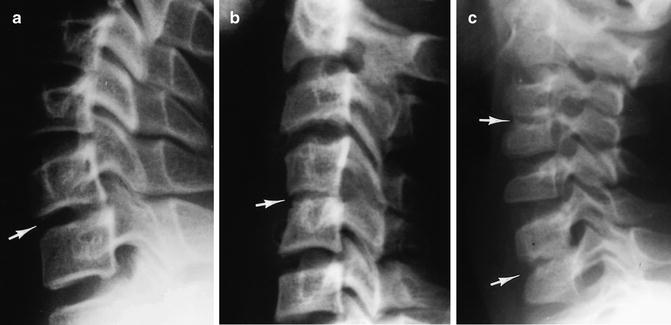
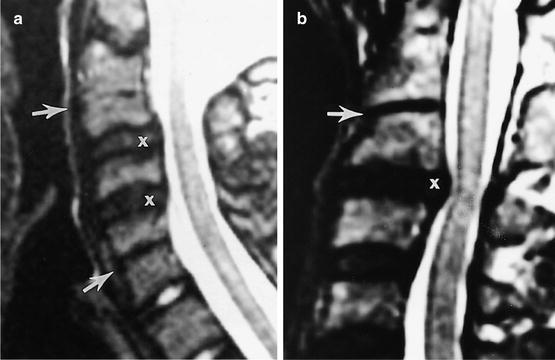
Fig. 3.3
Fusion C2–C3. Note fusion of the vertebral bodies of C2 and C3 (arrow). Fusion extends to the posterior elements; the neural arches and the spinous processes. There is only one spinous tip (cross symbol) for both C2 and C3
Fig. 3.4
Vertebral fusion: lower cervical spine. (a) Note the slightly narrowed intervertebral disk (arrow) between C6 and C7. (b) The disk (arrow) between the fused C4 and C5 cervical vertebrae is very narrow. Also note that the involved vertebrae are smaller than normal and taper toward the narrowed disk. (c) Fusions are present at both the C3–C4 and C6–C7 levels (arrows). The disk spaces are narrowed and almost obliterated. C3 and C4 are smaller than normal
Fig. 3.5
Vertebral fusion with hypertrophied intervertebral disks. (a) In this patient two levels of fusion (narrowed disks) are present (arrows). The large, hypertrophied intervening disks (cross symbols) bulge into the spinal canal but do not encroach upon the spinal cord. Note that the involved disks also have lost their normal high signal on this T2-weighted image. (b) In this patient there is fusion of C2 and C3 (arrow). The disk below is hypertrophied and bulges (cross symbol) into the spinal canal, causing slight compression of the spinal cord
C1 and C2 also can fuse, and often such fusion is associated with anomalous dens development (Fig. 3.6). This is important because while most cases of fusion at lower levels are not a clinical problem, this is not always true in the upper cervical spine: In the upper cervical spine, when there is enough associated anomalous formation, instability can be present (Fig. 3.7).
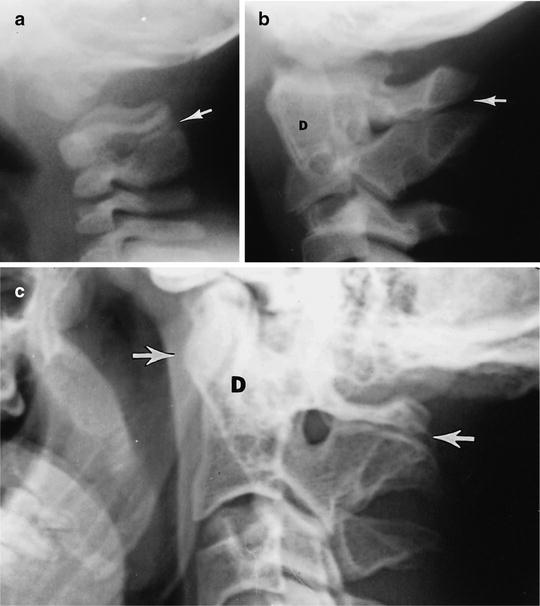
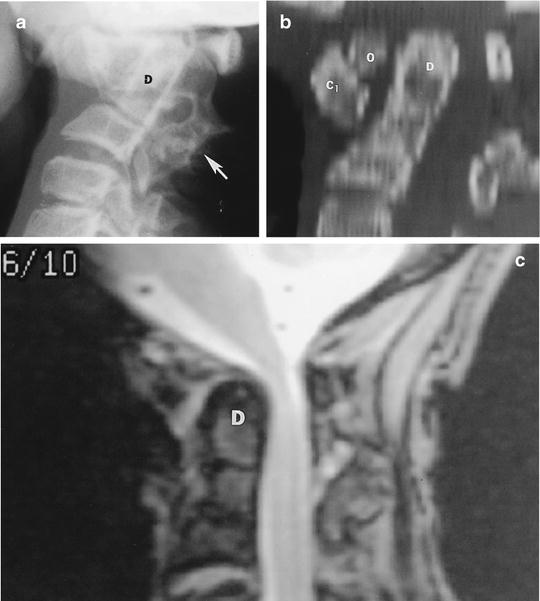
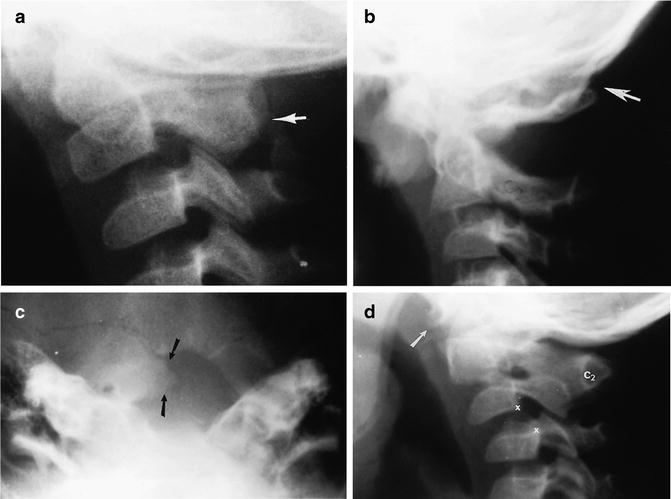
Fig. 3.6
C1–C2 fusion. (a) Note fusion of the posterior arches of C1 and C2 (arrow). (b) Older child demonstrating posterior fusion of C1 and C2 (arrow). The dens (D) is deformed, and there is no ossification of the anterior arch of C1. (c) In this patient there is anomalous formation of the fused neural arches of C1 and C2 (posterior arrow). The anterior arch of C1 is hypertrophied (anterior arrow) and the dens (D) is underdeveloped. The cervical spine in all these patients was stable
Fig. 3.7
Fusion: upper cervical spine with instability. (a) Note marked deformity and fusion of the posterior elements of C2 and C3 (arrow). The dens (D) is posteriorly tilted and slightly underdeveloped. The predental distance is increased. (b) Sagittal reconstructed CT study demonstrates the posteriorly tilted dens (D); here the wide predental distance seen in (a) is filled with a displaced os odontoideum (O). The anterior arch of C1 (C1) is deformed and overgrown. (c) Sagittal MR study demonstrates that the dens (D) is encroaching upon the spinal canal and causing compression of the upper cord
When fusion anomalies are extensive, and accompanied by segmentation (hemivertebra) anomalies, bizarre configurations are common. This most commonly occurs in the Klippel–Feil syndrome, but interestingly, even if the cervical spine appears very bizarre and distorted (Fig. 3.8), only seldom is neurologic deficit a problem. However, these patients also can have associated congenital deafness, renal anomalies, and Sprengel’s deformity (Fig. 3.9) of the scapula [3–5]. Neurologic deficit is more likely to occur in adulthood, and finally a rare form of severe fusion–segmentation abnormality occurs in usually lethal iniencephaly [6], a condition in which the underdeveloped upper cervical spine is fused to the occiput (Fig. 3.10).

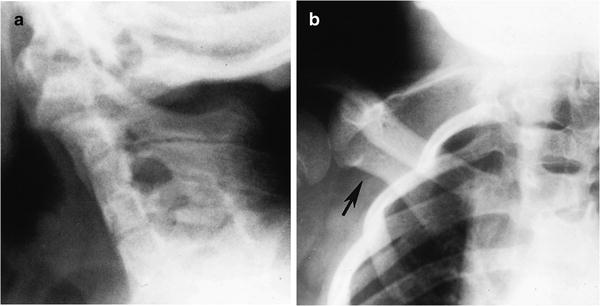

Fig. 3.8
Klippel–Feil syndrome. Note extensive fusion–segmentation anomalies of the entire cervical spine
Fig. 3.9
Klippel–Feil syndrome with Sprengel’s deformity. (a) Note extensive fusion–segmentation anomalies through both the vertebral bodies and posterior arches of the cervical spine. (b) Same patient. The right scapula is rotated and elevated (arrow), constituting Sprengel’s deformity
Fig. 3.10
Iniencephaly. (a) Note the underdeveloped, malformed cervical spine, which basically is fused with the occiput. The patient’s neck is held in extreme extension (Reproduced with permission from LE Swischuk, Imaging of the Newborn Infant and Young Child, Lippincott Williams & Wilkins, Baltimore, 1997)
Fusion of C1 to the base of the skull constitutes so-called occipitalization, and fusion can be complete, partial, unilateral, and either bony or fibrous (Fig. 3.11). In any of these cases, the uppermost neural arch is the largest one visible and thus should be the posterior arch of C2 (Fig. 3.11). Therefore, even though one does not come to the conclusion on initial inspection that C1 is fused with the base of the skull, the presence of this large uppermost neural arch and spinous process should provide the proper clue to the underlying diagnosis. Suspected occipitalization is easily confirmed with flexion views and CT of the cervical spine where the fused posterior arch of C1 is easier to assess (Fig. 3.12).
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
