(1)
Department of Pediatric Radiology, University of Texas Medical Branch, Galveston, TX, USA
Abstract
The den is critical to the upper cervical spine and has a complex developmental history. Very often normal anomalies and variations mimic pathology. This chapter is devoted to a detailed discussion of anomalies of the dens and how they can be differentiated from pathologic processes.
The Os Terminale–Os Odontoideum Complex
There always has been some disagreement about whether the os terminale and the os odontoideum are the same or different bones. However, I have always considered them to be the same, believing that the os terminale becomes the os odontoideum when it enlarges in association with hypoplasia of the dens [1]. This also has been suggested by others [2], and the concept is depicted in Fig. 4.1.
Fig. 4.1
Range of dens anomalies. Left to right: normal dens with a fused os terminale; normal dens with an unfused os terminale; hypoplastic dens with an enlarged unfused os terminale (now termed an os odontoideum); hypoplasia of the dens with no development of the os terminale; complete absence of the dens (Modified from von Torklus D, Gehle W. The Upper Cervical Spine: Regional Morphology, Pathology, and Traumatology; An X-Ray Atlas. New York: Grune & Stratton; 1972)
Embryologically, the os terminale is derived from the fourth occipital sclerotome and eventually fuses with the dens, as shown earlier in Fig. 4.1. If, on the other hand, the dens undergoes hypoplasia, the os terminale overgrows and becomes the os odontoideum (Fig. 4.1). What is important about all this is that the os odontoideum, as it enlarges, can assume an almost endless, and often very bizarre, variety of configurations. At the same time, there is underdevelopment of the ligaments stabilizing C1 and C2, and because of this the whole problem is associated with varying degrees of hypermobility and instability of C1 and C2, frequently requiring surgical stabilization.
The normal os terminale sits atop the dens in a V-shaped notch (Fig. 4.2), and in some cases its location is more posterior than anterior (Fig. 4.3). In some of these cases the os terminale is a little larger than usual. When the os terminale is seated deep within the notch of the dens, it is not seen on lateral view, but in other cases it sits well above the tip of the dens and appears as a single, smooth ossicle (Fig. 4.4a). In some of these cases the dens is a little dysplastic/deformed in appearance but not overtly hypoplastic (Fig. 4.4b). In other cases, especially on CT evaluation, confusing, but still normal, bony fragmentation of the dens may mimic a comminuted dens fracture (Fig. 4.5). In this regard, however, one might recall that extensively comminuted fractures of the tip of the dens are basically nonexistent.

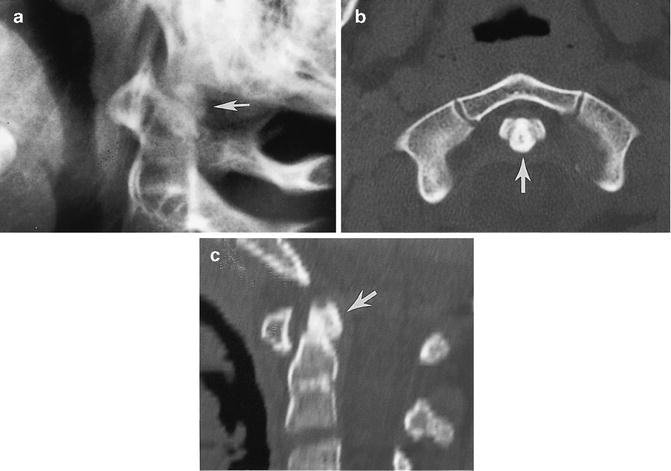
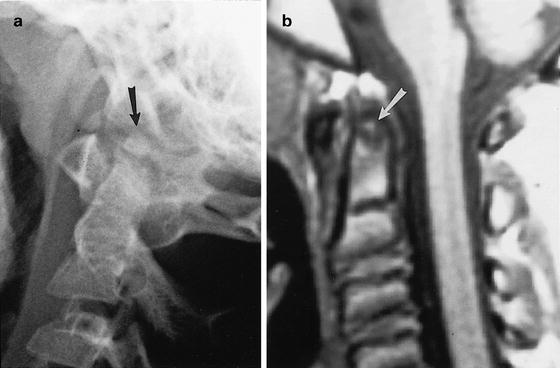
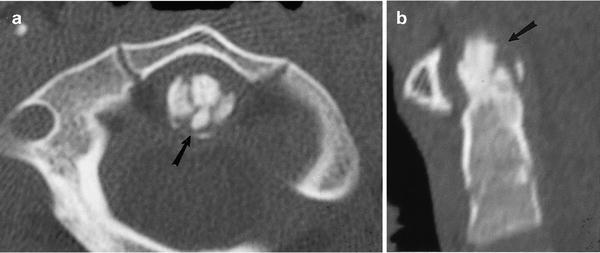
Fig. 4.2
Normal os terminale. (a) Note the os terminale (arrow) embedded into the V-shaped notch of the dens. (b) Similar findings; os terminale (arrow) on a coronally reconstructed CT study. (c) Sagittal CT reconstruction demonstrates the typical position of the os terminale (arrow). (d) Axial CT study demonstrates the usual central position of the os terminale (arrow)
Fig. 4.3
Normal os terminale: posterior position. (a) Slightly large, posteriorly located os terminale (arrow). (b) Axial CT study in another patient demonstrates the os terminale (arrow) to be slightly posterior in location. (c) Sagittal reconstruction view more clearly demonstrates the posterior location of the os terminale (arrow)
Fig. 4.4
Normal os terminale. (a) Note the normal os terminale (arrow), high sitting atop the normally developed dens. (b) Sagittal tomogram in another patient demonstrates the round os terminale (arrow) sitting atop the short dens
Fig. 4.5
Normal fragmented appearance of os terminale. (a) Axial CT study demonstrates a fragmented appearance to the os terminale and tip of the dens (arrow). (b) Sagittal reconstruction demonstrates similar findings (arrow) (From Swischuk et al. [1])
As noted earlier, when the dens becomes hypoplastic, the os terminale enlarges and overgrows to become the os odontoideum. The os odontoideum can be relatively small or very large, round or oval, or very bizarre and irregular in appearance. At any rate, when this complex of findings is seen the upper cervical spine becomes unstable (Figs. 4.6 and 4.7). Generally, if there is forward flexion motion of C1 on C2 greater than 2 mm, pathologic instability is present. Surgical stabilization is required, and this is important because many, of these cases are incidentally discovered in the Emergency Room when trauma to the head and/or cervical spine has been sustained. Therefore, while in some cases the findings may be minor and of no clinical consequence, in other instances significant instability of the upper cervical spine is present and the problem becomes just as great as if an unstable fracture were present.
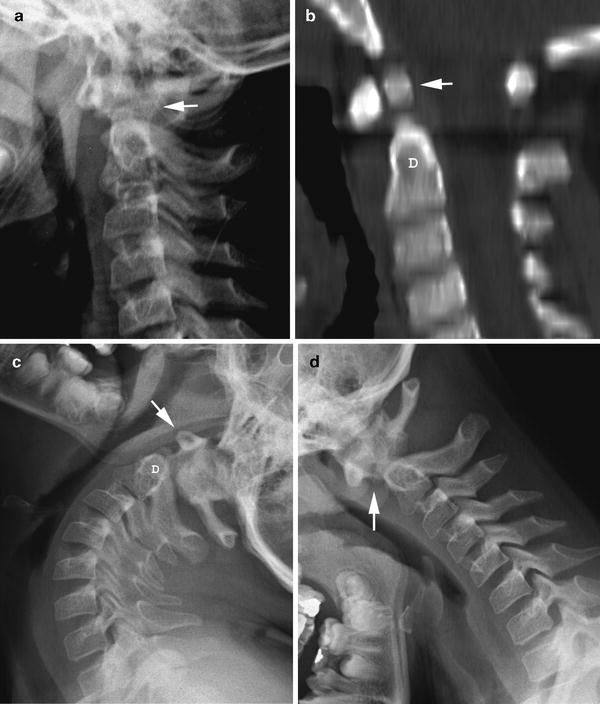
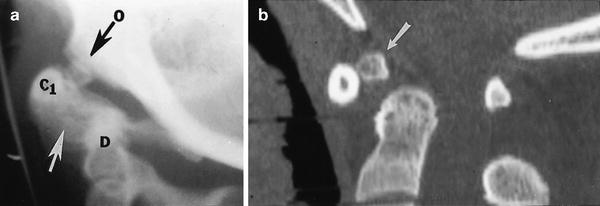




Fig. 4.6
Hypoplastic dens, os odontoideum, and hypermobility. (a) The dens is not clearly visualized (arrow). The reason is that it is hypoplastic. (b) Sagittal reconstructed CT image demonstrates the hypoplastic dens (D) and the os odontoideum (arrow). Note the relationship of the anterior arch of C1 to the dens. (c) With extension the anterior arch of C1 (arrow) comes to lie directly over the dens (D). (d) With flexion the anterior arch of C1 moves far forward and the space between it and the dens becomes markedly widened (arrow)
Fig. 4.7
Hypoplastic dens, os odontoideum, and hypermobility. (a) Note the markedly widened C1-dens distance (white arrow). The dens (D) is hypoplastic. C1 (C1) is slightly enlarged and the os odontoideum (O) is anteriorly dislocated. (b) Sagittal reconstructed CT study in another patient demonstrates findings similar to those seen in (a). Note the small, anteriorly displaced os odontoideum (arrow)
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
