VALVE DYSPLASIA, AND
TRICUSPID REGURGITATION
14
 EBSTEIN ANOMALY
EBSTEIN ANOMALY
Definition, Spectrum of Disease, and Incidence
In the normal heart the tricuspid valve inserts more apically on the interventricular septum than the mitral valve (see Chapter 5). In Ebstein anomaly the septal and posterior leaflets of the tricuspid valve are displaced inferiorly from the tricuspid valve annulus, toward the apex, and originate from the right ventricular myocardium (Figs. 14-1 and 14-2). The anterior tricuspid leaflet maintains its normal attachment to the tricuspid valve annulus. The proximal portion of the right ventricle is then continuous with the true right atrium and forms an “atrialized” portion of the right ventricle (Figs. 14-1 and 14-2). The spectrum of Ebstein anomaly is wide and varies from a minor form, with minimal displacement of the tricuspid valves with mild tricuspid regurgitation, to a severe form, with the “atrialization” of the entire right ventricle (Fig. 14-3).
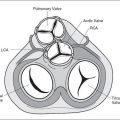
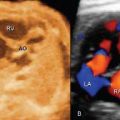
Associated anomalies are not uncommon and include right ventricular outflow tract obstruction, either as pulmonary stenosis (Fig. 14-4) or atresia, and atrial and ventricular septal defects. The pathogenesis of pulmonary stenosis or atresia in association with Ebstein anomaly may be related to a reduction in flow across the pulmonary valve due to severe tricuspid regurgitation. Atrial septal defect may also result from the dilation of the right atrium due to the severe regurgitation noted in utero. Ebstein anomaly is one of the less common cardiac abnormalities occurring in about 0.5% of congenital heart disease in the neonate, with an equal male-to-female distribution (1,2). Ebstein anomaly is more common in prenatal series as it accounts for 3% to 7% of congenital heart disease in fetuses (3,4). This higher prenatal rate is related to an increase in fetal or early neonatal death in severe cases due to severe tricuspid regurgitation and associated pulmonary hypoplasia.
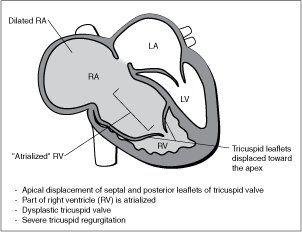
Figure 14-1. Ebstein anomaly. RA, right atrium; LA, left atrium; LV, left ventricle.
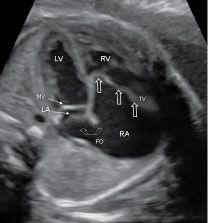
Figure 14-2. Four-chamber view in a fetus with Ebstein anomaly demonstrating the typical apical displacement of the tricuspid valve (TV) (open straight arrows) compared to the mitral valve (MV). The right atrium (RA) is dilated due to severe TV regurgitation, and the interatrial communication through the foramen ovale (FO) is wide (open curved arrow) due to increased right-to-left shunting of blood. LV, left ventricle; RV, right ventricle; LA, left atrium.
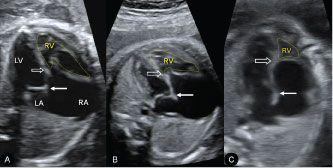
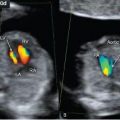
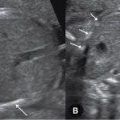
Figure 14-3. Spectrum of disease in Ebstein anomaly. Septal attachment and displacement of the tricuspid valve differs as shown in three fetuses (A–C) with Ebstein anomaly. A–C show increasing distance between the attachment of the tricuspid valve (open arrow) and the mitral valve (solid arrow). The atrialized portion of the right ventricle (RV) is biggest with more apical tricuspid valve displacement (C). RA, right atrium; LA, left atrium; LV, left ventricle.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


