Fig. 12.1
Parasternal long-axis end-systolic image at rest, demonstrating posterior mitral valve leaflet prolapse
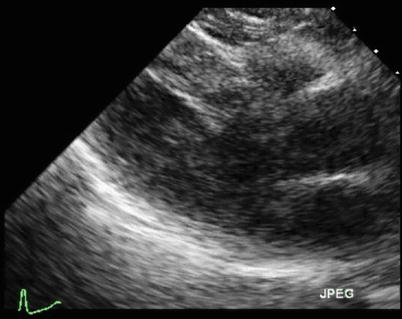
Fig. 12.2
Parasternal long-axis end-systolic image at peak exercise. Note the decreased left ventricular cavity size

Fig. 12.3
Parasternal short-axis end-systolic image at rest

Fig. 12.4
Parasternal short-axis end-systolic image at peak exercise. Note the decreased left ventricular cavity size
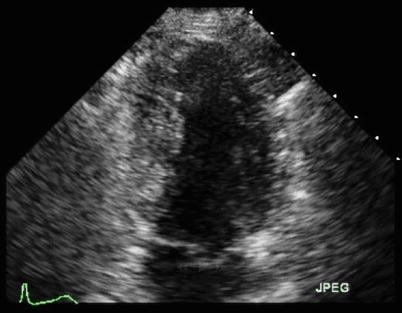
Fig. 12.5
Apical two-chamber end-systolic image at rest

Fig. 12.6
Apical two-chamber end-systolic image at peak exercise. Note the decreased left ventricular cavity size
Video 12.1 Parasternal long-axis end-systolic image at rest, demonstrating posterior mitral valve leaflet prolapse (AVI 1240 kb)
Video 12.2 Parasternal long-axis end-systolic image at peak exercise. Note the decreased left ventricular cavity size (AVI 892 kb)
Video 12.3 Parasternal short-axis end-systolic image at rest (AVI 1241 kb)
Video 12.4 Parasternal short-axis end-systolic image at peak exercise. Note the decreased left ventricular cavity size (AVI 932 kb)
Video 12.5 Apical two-chamber end-systolic image at rest (AVI 1273 kb)
Video 12.6 Apical two-chamber end-systolic image at peak exercise. Note the decreased left ventricular cavity size (AVI 849 kb)
12.2 Case 2. Impaired Contractile Reserve: Increased Left Ventricular Size with Stress
A 52-year-old previously fit ballet instructor with known mitral valve prolapse and significant MR presented with increasing fatigue but no overt dyspnea or signs of heart failure. She was referred for exercise stress echocardiography to assess left ventricular contractile reserve and exercise capacity. She achieved 8 min of treadmill exercise according to the standard Bruce protocol. The test was ceased at 92 % of the maximum predicted heart rate because of dyspnea and fatigue.
Regional wall motion analysis did not demonstrate any focal abnormalities to suggest inducible ischemia, but the left ventricular size remained unchanged at peak exercise. This failure of augmentation in left ventricular function at peak stress reflected impaired contractile reserve. Color Doppler imaging also demonstrated a significant increase in the severity of her MR at peak stress. She was referred for consideration of mitral valve surgical repair.
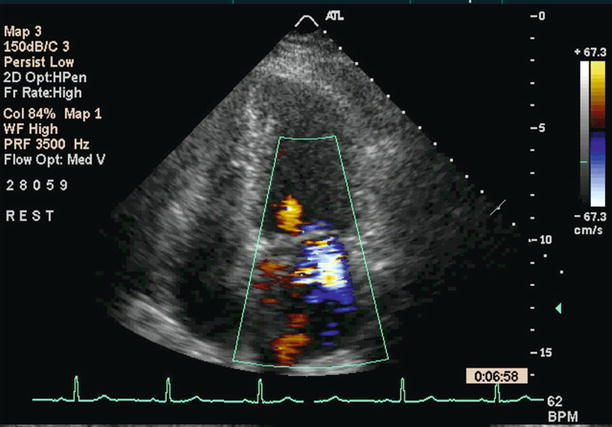
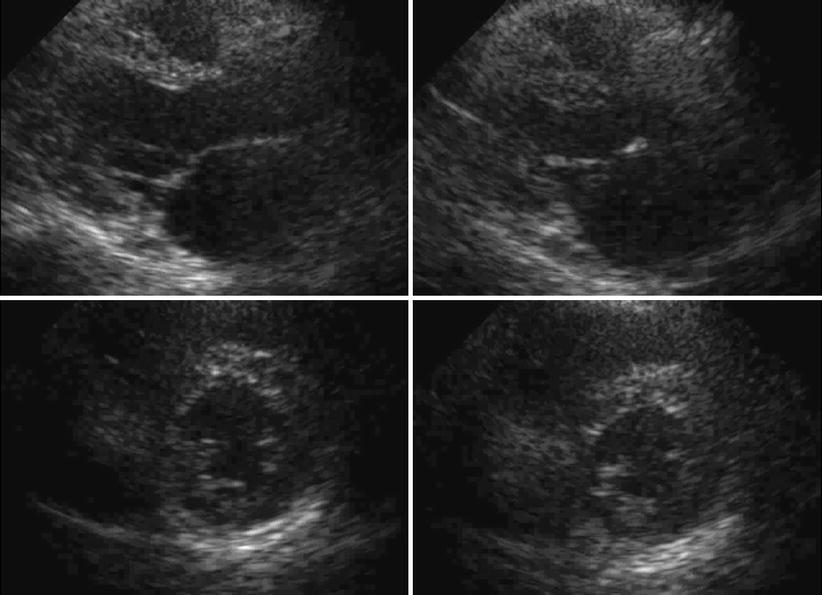
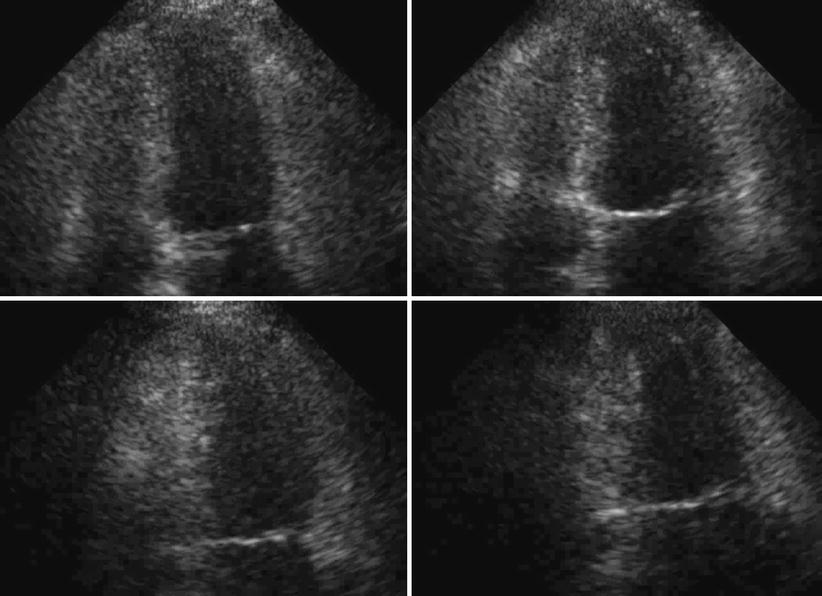
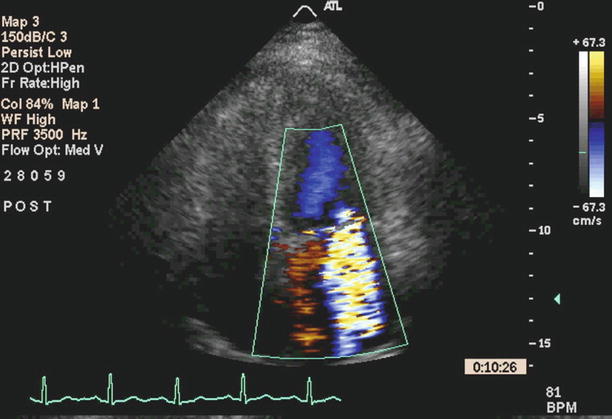
Fig. 12.7
Apical four-chamber view with color Doppler demonstrating moderate (2+) mitral regurgitation at baseline (heart rate 62 bpm)
Fig. 12.8
Parasternal stress echocardiographic images before exercise (left images) and after exercise (right images). The images at the top show the long-axis view and the bottom images show the short-axis view at the level of the mid left ventricle. The left ventricular cavity increases with exercise stress, consistent with impaired contractile reserve
Fig. 12.9
Apical four-chamber (top) and two-chamber (bottom) stress echocardiographic images before exercise (left images) and after exercise (right images). The left ventricular cavity size increases with exercise stress, consistent with impaired contractile reserve
Fig. 12.10
Apical four-chamber view with color Doppler demonstrating severe (4+) mitral regurgitation in the early recovery phase even though the heart rate had nearly returned to the baseline of 68 bpm
Video 12.7 Apical four-chamber view with color Doppler demonstrating moderate (2+) mitral regurgitation at baseline (heart rate 62 bpm) (MOV 454 kb)
Video 12.8 Parasternal stress echocardiographic images before exercise (left images) and after exercise (right images). The images at the top show the long-axis view and the bottom images show the short-axis view at the level of the mid left ventricle. The left ventricular cavity increases with exercise stress, consistent with impaired contractile reserve (AVI 1799 kb)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree