Clinical Presentation
The patient is a 72-year-old female with longstanding gait disturbance, spasticity, back pain, right hip pain, and lower extremity hyperreflexia. No bowel or bladder dysfunction. No thoracic sensory level. Based on clinical findings, obtained lumbar magnetic resonance (MR) study to rule out lumbar disc herniation, which was negative. Obtained additional thoracic and cervical MR studies because of hyperreflexia.
Imaging Presentation
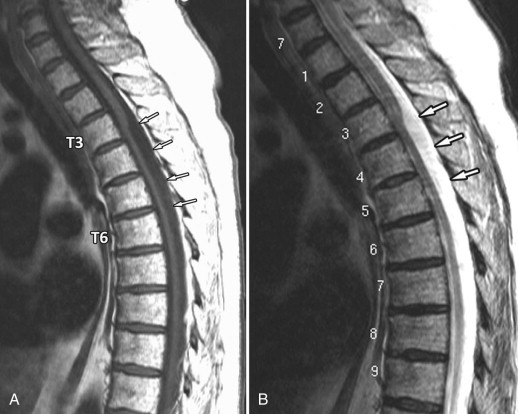
Thoracic MR study revealed a fusiform T1 hypointense, T2 hyperintense fluid collection within the thecal sac displacing the spinal cord anteriorly from the C3 level to approximately the C6 level consistent with a posterior arachnoid cyst ( Figs. 9-1 and 9-2 ) .

Discussion
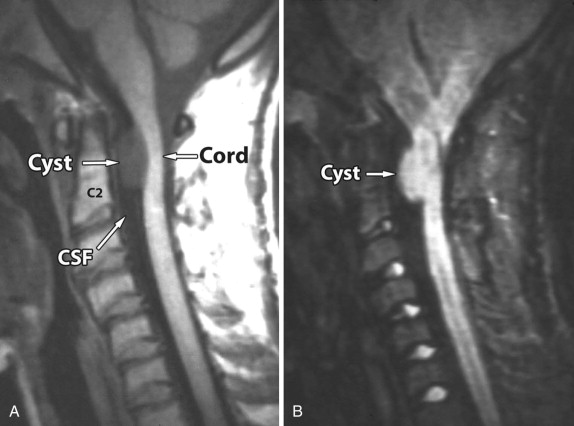
Spinal arachnoid cysts are uncommon. They are intradural-extramedullary or extradural collections of cerebrospinal fluid (CSF)–like fluid, most commonly occurring in the thoracic spinal canal dorsal to the thoracic spinal cord. Intradural arachnoid cysts are less common than extradural arachnoid cysts ( Figs. 9-3 and 9-4 ) . Patients with arachnoid cysts usually present between the ages of 20 and 50, but these cysts can occur at any age and any spinal level ; 85% are located in the thoracic spinal canal, 15% in the cervical spinal canal ( Figs. 9-5 and 9-6 ) , and 5% in the lumbar spinal canal. The majority of spinal arachnoid cysts are located dorsal to the spinal cord (see Fig. 9-1 ).



Primary (congenital) arachnoid cysts are almost always intradural and represent meningeal duplication cysts where the arachnoid layer, comprised of two layers of cuboidal epithelium, is split into two layers by the fluid collection, so the wall of the arachnoid cyst is lined by a single layer of cuboidal epithelium. Primary arachnoid cysts are almost always located dorsal to the cord. A hydrodynamic theory has been postulated regarding the formation of arachnoid cysts in which CSF pulsation is said to expand congenitally weakened areas in the arachnoid. Posterior intradural arachnoid cysts are believed to arise in the region of the septum posticum of Schwalbe. Secondary (acquired) arachnoid cysts (also called subarachnoid cysts ) may occur after trauma, hemorrhage, surgery, or infection (arachnoiditis), and are believed to be secondary to developing adhesions, which can result in loculation of a CSF collection. Secondary arachnoid cysts may be intradural or extradural.
Spinal arachnoid cysts are a type of meningeal cyst, which have been classified by Naybors and colleagues. Type 1 cysts are spinal extradural meningeal cysts without spinal nerve root fibers (see Fig. 9-2 ). Type 2 meningeal cysts are spinal extradural meningeal cysts with spinal nerve root fibers. Type 3 cysts are spinal intradural meningeal cysts (see Fig. 9-1 ). Type 2 meningeal cysts include the common Tarlov-type perineural cysts (spinal nerve root diverticula) that frequently occur within the spinal or sacral neural foramina.
Patients with arachnoid cysts can present with back pain or be myelopathic with hyperreflexia, paraparesis, paresthesias, or bladder/bowel incontinence. Radiculopathy can also occur. Ventral cysts are more likely to cause weakness and myelopathic signs. Some patients with arachnoid cysts are asymptomatic; the cysts are discovered incidentally on thoracic MR studies performed for other reasons. Back pain is the most common manifesting complaint, followed by sensory changes, urinary incontinence, and weakness. An intermittent waxing and waning clinical course is typical, which clinically may simulate multiple sclerosis. Postural changes can accentuate or alleviate the symptoms. Cyst enlargement is attributed to the presence of a ball-valve–type obstruction allowing CSF to flow into but not out of the cyst. Pain associated with arachnoid cysts may be accentuated during the Valsalva maneuver. If the arachnoid cyst is not removed, the adjacent spinal cord may become atrophic. Arachnoid cysts may be associated with scoliosis, syringohydromyelia and rarely spinal dysraphism (meningomyelocele or diastematomyelia). If an associated syringohydromyelia occurs, the syrinx typically extends above the level of the cyst. Arachnoid cysts have no malignant potential.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


