Presentation and Presenting Images
( ▶ Fig. 33.1, ▶ Fig. 33.2, ▶ Fig. 33.3, ▶ Fig. 33.4)
A 54-year-old female who has had prior benign biopsies and surgical excisions of the left breast presents for screening mammography.
33.2 Key Images
33.2.1 Breast Tissue Density
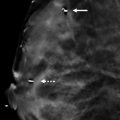
The breasts are heterogeneously dense, which may obscure small masses.
33.2.2 Imaging Findings
There is a subtle area of architectural distortion in the left breast at the 12 o’clock location in the posterior depth, best seen in the digital breast tomosynthesis (DBT) images ( ▶ Fig. 33.5 and ▶ Fig. 33.6). There is a dumbbell-shaped biopsy clip in the upper outer quadrant from a prior remote benign breast biopsy.
33.3 BI-RADS Classification and Action
Category 0: Mammography: Incomplete. Need additional imaging evaluation and/or prior mammograms for comparison.
33.4 Diagnostic Images
( ▶ Fig. 33.7, ▶ Fig. 33.8, ▶ Fig. 33.9, ▶ Fig. 33.10, ▶ Fig. 33.11, ▶ Fig. 33.12)
33.4.1 Imaging Findings
The diagnostic imaging ( ▶ Fig. 33.7 and ▶ Fig. 33.8) demonstrates persistent very subtle architectural distortion, which is much more evident on the DBT images. A scar marker was placed on the skin incision scar. The surgical site appears to be more lateral to the area of architectural distortion. An ultrasound was performed and identified two areas at the 11 o’clock location. The area 2 cm from the nipple appears as an irregular hypoechoic mass with indistinct margins located within dense fibroglandular tissue ( ▶ Fig. 33.9). The area 5 cm from the nipple appears to be an irregular mixed echogenicity mass with indistinct margins and with solid and cystic components ( ▶ Fig. 33.10). Biopsy was performed on both masses identified on ultrasound. The lesion at 2 cm from the nipple was marked with a ribbon biopsy marker, and the lesion at 5 cm from the nipple was marked with a coil biopsy marker ( ▶ Fig. 33.11 and ▶ Fig. 33.12).
33.5 BI-RADS Classification and Action
Category 4A: Low suspicion for malignancy
33.6 Differential Diagnosis
Radial scar: The ribbon marker appears closest to the area of architectural distortion mammographically. The diagnosis was radial scar and fibrocystic changes. The diagnosis for the area marked by the coil marker was hyalinized breast stroma.
Surgical scar: It can be difficult even with DBT in dense breast tissue to differentiate between surgical scars and new findings when they are in close proximity to each other.
Breast cancer: Breast cancer can present as an architectural distortion. This would have been a concordant diagnosis at biopsy.
33.7 Essential Facts
Radial scars are benign lesions that are often classified as high risk due to the variety of proliferative lesions that can be associated with them.
Histologically radial scars have a central sclerotic core from which radiates the proliferative lesions.
Radial scars range in size form microscopic incidental lesions to larger macroscopic lesions seen mammographically, which are indistinguishable from malignancies.
Architectural distortion is not a very common imaging finding. Radial scars are the most common benign cause for architectural distortion.
33.8 Management and Digital Breast Tomosynthesis Principles
Architectural distortion accounts for 12 to 45% of missed breast cancers.
Architectural distortion is often better seen on DBT than on conventional digital mammography. Radial scars are a subset of the lesions that present as architectural distortion . Controversy remains on whether to manage radial scars with excision or observation; additional data is needed to guide management of radial scars only visible on DBT.
Architectural distortion is the mammographic finding with the lowest interobserver agreement between radiologists.
33.9 Further Reading
[1] Partyka L, Lourenco AP, Mainiero MB. Detection of mammographically occult architectural distortion on digital breast tomosynthesis screening: initial clinical experience. AJR Am J Roentgenol. 2014; 203(1): 216‐222 PubMed
[2] Ray KM, Turner E, Sickles EA, Joe BN. Suspicious Findings at Digital Breast Tomosynthesis Occult to Conventional Digital Mammography: Imaging Features and Pathology Findings. Breast J. 2015; 21(5): 538‐542 PubMed

Fig. 33.1 Left cranicaudal (LCC) mammogram.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


