Presentation and Presenting Images
( ▶ Fig. 79.1, ▶ Fig. 79.2, ▶ Fig. 79.3, ▶ Fig. 79.4, ▶ Fig. 79.5, ▶ Fig. 79.6, ▶ Fig. 79.7, ▶ Fig. 79.8, ▶ Fig. 79.9)
A 47-year-old female with two palpable abnormalities marked with BBs presents for mammographic evaluation. She has a history of a benign left breast duct excision.
79.1.1 Breast Tissue Density
There are scattered areas of fibroglandular density.
79.1.2 Imaging Findings
The conventional digital mammograms and digital breast tomosynthesis (DBT) images did not reveal any findings to correspond to the two palpable findings marked with BBs at the 12 o’clock and 5 o’clock locations on the left breast ( ▶ Fig. 79.1, ▶ Fig. 79.2, ▶ Fig. 79.3, ▶ Fig. 79.4, ▶ Fig. 79.5, ▶ Fig. 79.6, ▶ Fig. 79.7, ▶ Fig. 79.8, and ▶ Fig. 79.9). . The DBT images demonstrate an area of architectural distortion at the 10 o’clock location ( ▶ Fig. 79.5 and ▶ Fig. 79.6). An ultrasound was recommended to further evaluate the palpable findings and the area of architectural distortion at the 10 o’clock location.
79.2 Diagnostic Images
( ▶ Fig. 79.10; ▶ Fig. 79.11; ▶ Fig. 79.12; ▶ Fig. 79.13; ▶ Fig. 79.14; ▶ Fig. 79.15; ▶ Fig. 79.16)
79.2.1 Imaging Findings
The ultrasound of the palpable findings at the 12 o’clock and 5 o’clock locations revealed normal breast tissue (not shown). Corresponding to the area of architectural distortion noted at the 10 o’clock location on the DBT images, there is 8mm × 8mm × 7mm irregular mass with angular margins and posterior shadowing, 5 cm from the nipple ( ▶ Fig. 79.10 and ▶ Fig. 79.11). Due to the complexity of the imaging findings, the clinical history of a prior surgical excision, and the palpable findings, a BB marker was placed on the skin overlying the area of ultrasound abnormality. A repeat CC image was taken with the nipple in profile. The BB marker appears to correlate to the area of architectural distortion on the DBT ( ▶ Fig. 79.12). The lesion was biopsied with ultrasound guidance. The ribbon biopsy marker clip is located in the area of architectural distortion best seen on DBT ( ▶ Fig. 79.13 and ▶ Fig. 79.14). Enlarging the area of concern on the initial DBT images suggests that the architectural distortion is fatty, or radiolucent, in the center ( ▶ Fig. 79.15 and ▶ Fig. 79.16).
79.3 BI-RADS Classification and Action
Category 4C: High suspicion for malignancy
79.4 Differential Diagnosis
Invasive ductal carcinoma(IDC): The architectural distortion and irregular mass with indistinct margins are worrisome for an invasive carcinoma. The biopsy yielded grade 2 IDC with lobular features..
Radial scar/radial sclerosing lesion: The central area of the architectural distortion is more radiolucent, which has been reported as a sign in radial sclerosing lesions. This finding is not unique to radial scars. A biopsy is warranted.
Postoperative scar: The patient has had a prior duct excision. The skin marker denotes the surgical scar. This scar is in the inferior region of the breast and the area of concern is located in the upper inner quadrant; thus, the surgical scar is a much less likely cause of the finding. It is important to correlate skin incision scars and surgical reports to the imaging findings.
79.5 Essential Facts
Positioning remains important even for DBT. The initial craniocaudal (CC) view with the nipple not in profile obscures the visualization of this lesion ( ▶ Fig. 79.1). The repeat CC view without DBT demonstrates the lesion better ( ▶ Fig. 79.12). This lesion may have been better seen on a repeat CC DBT.
When a patient presents with a palpable finding or other clinical concern, it is important to evaluate that concern completely. However, it is just as important to evaluate the rest of the mammographic imaging and not become distracted by the area of clinical concern. This includes both breasts if both were imaged.
The presence or absence of fat within a lesion on DBT is not predictive of benignity or malignancy.
Cancers, due to their much faster growth rates compared to other tissue, may engulf fat as they grow and thus contain fat. This is in contrast to fat-containing benign masses, which are composed of fat and are surrounded by a thin capsule or pseudocapsule.
It is important to evaluate the margins of a mass on DBT.
79.6 Management and Digital Breast Tomosynthesis Principles
DBT’s ability to reconstruct the breast tissue into slices provides a look inside of masses.
DBT may reveal the presence of fat within a lesion that is not detected on conventional mammography.
Both benign and malignant masses may contain fat. With DBT, it may be possible to make a clearer distinction and thus avoid unnecessary biopsies, only biopsying those lesions that warrant it.
All spiculated fat-containing masses detected on DBT should be evaluated. The range of diagnosis for this finding is carcinoma, surgical scars, and fat necrosis. Historical information from the patient will be helpful in narrowing the diagnosis.
79.7 Further Reading
[1] Freer PE, Wang JL, Rafferty EA. Digital breast tomosynthesis in the analysis of fat-containing lesions. Radiographics. 2014; 34(2): 343‐358 PubMed
[2] Noroozian M, Hadjiiski L, Rahnama-Moghadam S, et al. Digital breast tomosynthesis is comparable to mammographic spot views for mass characterization. Radiology. 2012; 262(1): 61‐68 PubMed
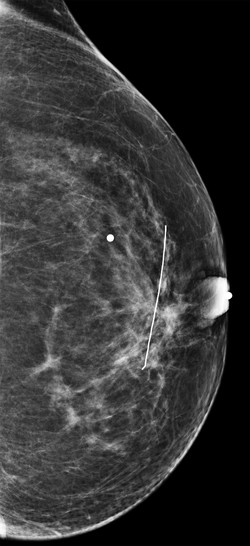
Fig. 79.1 Left craniocaudal (LCC) mammogram.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


