Presentation and Presenting Images
( ▶ Fig. 52.1, ▶ Fig. 52.2, ▶ Fig. 52.3, ▶ Fig. 52.4)
A 51-year-old female with history of right breast cancer treated with a lumpectomy and more recently a bilateral reduction mammoplasty presents for screening mammography.
52.2 Key Images
( ▶ Fig. 52.5, ▶ Fig. 52.6, ▶ Fig. 52.7, ▶ Fig. 52.8)
52.2.1 Breast Tissue Density
There are scattered areas of fibroglandular density.
52.2.2 Imaging Findings
There are postsurgical changes in the right breast consistent with the patient’s lumpectomy, the location of which is marked by the surgical clips at the 9 o’clock location in the posterior depth ( ▶ Fig. 52.1 and ▶ Fig. 52.3). There are bilateral changes due to the bilateral reduction surgery. In the left breast, there is a new mass located at the 7 o’clock location in the middle depth ( ▶ Fig. 52.5 and ▶ Fig. 52.6). This appears to be associated with the skin and is well demonstrated on the digital breast tomosynthesis (DBT) images. Note that it is located on slice 1 of the craniocaudal (CC) tomosynthesis image ( ▶ Fig. 52.7 and ▶ Fig. 52.8). No mention of a skin lesion was noted in the technologist’s intake sheet and no skin marker was placed on a skin lesion.
52.3 BI-RADS Classification and Action
Category 0: Mammography: Incomplete. Need additional imaging evaluation and/or prior mammograms for comparison.
52.4 Diagnostic Images
( ▶ Fig. 52.9, ▶ Fig. 52.10, ▶ Fig. 52.11)
52.4.1 Imaging Findings
The diagnostic images were taken after a skin marker was placed on the skin lesion (ring in ▶ Fig. 52.9, ▶ Fig. 52.10, and ▶ Fig. 52.11). The prior mass seen on the screening mammography and DBT examinations is related to a skin lesion. The patient had a regular follow-up appointment at the breast clinic on the same date as the diagnostic imaging. The clinical notes indicate that this skin lesion is located on the medial aspect of the reduction scar and was likely a “stitch cyst.”
52.5 BI-RADS Classification and Action
Category 2: Benign
52.6 Differential Diagnosis
Suture granuloma: Suture granulomas are benign granulomatous proliferations in response to a retained foreign body (suture material). They are less common with absorbable sutures but may still occur. They can occur anywhere along the suture line.
Epidermal inclusion cyst: These benign skin lesions can occur anywhere on the hair-bearing areas of the body. They are filled with laminated keratin, and can occur at the site of an obstructed hair follicle or pore and secondary to traumatic implantation of torn epidermis. This would be a reasonable diagnosis for this imaging finding.
Carcinoma: This is less likely. Carcinoma can occur at suture lines but this tends to be in advanced cancers without clear surgical margins or as a late recurrence of cancer.
52.7 Essential Facts
Many skin lesions can simulate masses on mammography. Having knowledge and awareness of these skin based lesions is especially helpful to prevent unnecessary patient recalls.
Many skin lesions have characteristic mammographic and sonographic appearances.
The most common skin-based lesions are epidermal inclusion cysts and/or sebaceous cysts, moles and keratosis, and surgical scars. Patients with neurofibromatosis can also display skin lesions; however, this is less common.
It is extremely helpful to have dominant skin lesions marked with skin markers prior to mammographic imaging. Some patients have a large number of skin lesions, and therefore marking all of them can be disruptive to image interpretation.
When in question, it may require recalling a patient to determine if a lesion close to the skin surface on the mammogram is a skin lesion or a true parenchymal lesion.
52.8 Management and Digital Breast Tomosynthesis Principles
Tomosynthesis can be used to distinguish lesions that are located in the skin.
When a “lesion” is seen on the first or last image of a tomosynthesis movie, it is highly likely that this is a skin-based lesion. Making this observation can prevent recalling a patient for additional imaging. In this case, the skin lesion was seen on slice 1 of the CC tomosynthesis movie.
52.9 Further Reading
[1] Kim HS, Cha ES, Kim HH, Yoo JY. Spectrum of sonographic findings in superficial breast masses. J Ultrasound Med. 2005; 24(5): 663‐680 PubMed
[2] Rettenbacher T, Macheiner P, Hollerweger A, Gritzmann N, Weismann C, Todoroff B. Suture granulomas: sonography enables a correct preoperative diagnosis. Ultrasound Med Biol. 2001; 27(3): 343‐350 PubMed

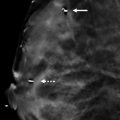
Fig. 52.1 Right craniocaudal (RCC) mammogram.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


