18
 COMMON ARTERIAL TRUNK
COMMON ARTERIAL TRUNK
Definition, Spectrum of Disease, and Incidence
Common arterial trunk (CAT), also referred to as persistent truncus arteriosus, truncus arteriosus communis, and aorticopulmonary trunk, is characterized by a single arterial trunk that arises from the base of the heart and gives origin to the systemic, coronary, and pulmonary circulations (Fig. 18-1). A large ventricular septal defect (VSD) is almost always present in this anomaly. CAT results from failure of the truncus swellings, which normally divide the truncus arteriosus into the aorta and pulmonary arteries during embryogenesis, to fuse, resulting in a persistent common trunk (1). The spectrum of the disease is wide and is mainly related to the anatomic origin of the right and left pulmonary arteries, which may arise from a pulmonary trunk (Fig. 18-1A,B) or as direct branches from the CAT or the descending aorta. CAT is classified into four types by Collett and Edwards, based on the anatomic origin of the pulmonary arteries (2). In type 1, a short pulmonary trunk arises from the CAT and divides into right and left pulmonary arteries (Fig. 18-1A). In types 2 and 3, both pulmonary arteries arise separately, as individual branches, from the CAT and they are either close anatomically (type 2) or at some distance from one another (type 3). In type 4, which is now reclassified as pulmonary atresia with VSD (see Chapter 17) rather than CAT, the pulmonary arteries arise from the aortic arch or the descending aorta. Another classification, type A1 through A4, is proposed by Van Praagh and Van Praagh (3). In this classification, type A1 is similar to type 1 of Collett and Edwards’s
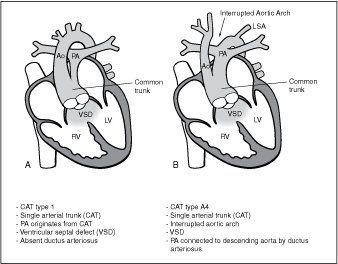
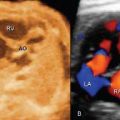
Figure 18-1. Common arterial trunk (CAT) type 1 (A) and type A4 (B). RV, right ventricle; LV, left ventricle; PA, pulmonary artery; Ao, aorta; LSA, left subclavian artery; VSD, ventricular septal defect.
classification, type A2 combines types 2 and 3, type A3 describes a single pulmonary artery origin from the CAT with either a ductus or collateral circulation supplying the contralateral lung, and type A4 refers to abnormalities of the aortic arch including complete interruption (Fig. 18-1B). The root of the CAT is large and has a biventricular origin in most cases. In up to a third of CAT cases, however, the root appears to arise entirely from the right ventricle, and in rare cases entirely from the left ventricle. The CAT valve has three leaflets (tricuspid) in about 69% of cases, four leaflets (quadricuspid) in 22% of cases, two leaflets (bicuspid) in 9% of cases, and, on very rare occasions, one, five, or more leaflets (4). The two most commonly diagnosed types of CAT in the fetus are type 1/type A1 and type A4. Figure 18-2 shows an anatomic specimen of CAT type 1.
CAT is found in 1.6% of all newborns with congenital heart disease (5), is reported to occur in about 1.07 of 10,000 births (6), and is found more commonly in offsprings of diabetic mothers (7). CAT occurs equally in boys and girls and is more commonly prevalent in fetal series (8). Associated chromosomal anomalies, mainly deletion 22q11, are common.
Ultrasound Findings
Gray Scale
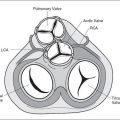
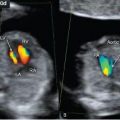
The four-chamber view appears normal in CAT (Fig. 18-3A) unless the VSD is large and visible in this plane or levorotation of the heart is present. The diagnosis is best achieved by detecting a malaligned VSD with an overriding large vessel on the five-chamber view (Fig. 18-3B) and an absence of a separate pulmonary artery and valve arising from the right ventricle. Confirming the diagnosis is usually made by identifying the pulmonary trunk (or arteries) directly arising from the overriding large vessel (Fig. 18-3B). In the five-chamber view, the root of the CAT is large and the valve leaflets are thickened (dysplastic) with lack of proper excursion (Fig. 18-4). Short-axis view may demonstrate an abnormal number of valve leaflets (Fig. 18-5). Identifying a short main pulmonary artery in the five-chamber view that arises from the large common trunk and courses to the left confirms the CAT diagnosis (type 1) and differentiates this abnormality from tetralogy of Fallot. In CAT type 1, the aorta is large and the pulmonary artery is narrow. In the CAT types 2 and 3, there is no pulmonary trunk, and the pulmonary arteries arise either posteriorly (type 2) or laterally (type 3) from the common trunk. Differentiating various CAT types is difficult and unreliable prenatally, especially in the second trimester (9). The three-vessel-trachea view is also helpful in
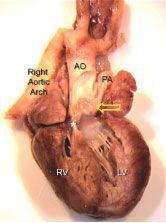
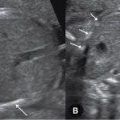
Figure 18-2. Anatomic specimen of common arterial trunk type 1 (compare to Fig. 18-1A). The common trunk (arrow) is open to demonstrate the dysplastic truncal valve and the bifurcation into the pulmonary artery (PA) and the aorta (AO). The ductus arteriosus is absent and a right aortic arch is noted. The asterisk shows a ventricular septal defect. RV, right ventricle; LV, left ventricle.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


